

This post provides a brief overview of ketamine, the pharmacology, mechanism of action, and its medicinal and recreational use. Ketamine is of one of the most unique and versatile synthetic drugs and new applications are still emerging.

Ketamine was first synthesized by chemists at the Parke Davis company in 1956. They had been working to develop new anesthetic agents the first of which to gain approval was the related agent phencyclidine, PCP. That drug was discontinued some years later as it became popular as an illicit drug known as “angel dust” and due to unwanted side effects.
Ketamine, a similar compound was discovered to produce profound anesthesia with less emergence delirium and was approved for clinical use in 1970. Early clinical trials published in 1966 revealed that ketamine had anesthetic and analgesic properties suitable for surgical procedures. It is short acting and safe to administer producing no significant respiratory depression at effective doses.
Ketamine exists in two isomeric forms R- and S- isomers with differing properties. It is primarily produced as the mixed salts. Esketamine produced as a nasal inhaler is the R form of Ketamine. The drug is classified as schedule III by the FDA, meaning approved for general medical use with significant abuse potential.
Ketamine is readily soluble in water and lipids contributing to its bio active properties.

Ketamine was developed and marketed as an anesthetic which could be used as a primary agent or as an adjunct to general anesthetics. It has strong pain relieving properties. Ketamine produces a unique state referred to as dissociative anesthesia. At high doses the patient will seem to be awake however will not respond to sensory stimuli and not form memories of the event.
The drug was put into use soon after initial trials by the US military for use in front line combat medical treatment in the Vietnam war. Unlike morphine or other agents it does not require intubation or respiratory support and has a high safety profile. It could be administered in the field or en route to field hospitals.
With this extensive real world experience ketamine quickly found use in surgical anesthesia, as a sedative hypnotic in short term interventions, and as an analgesic for refractory pain. It’s use for these indications is less common now due to use of other drugs such as propofol.
Psychoactive effects are dose dependent. In lower doses it produces euphoria similar to other psychoactive drugs. Users may experience mild dissociation along with visual or auditory hallucinations and distorted sense of time and place. Referential delusions and thought disorder may occur. While a limiting factor in clinical use these are desired effects in recreational use.
Higher doses may produce schizophrenia like symptoms with dissociation and out-of-body like effects. These generally resolve with a few hours with no residual effects.
Recreational use is common as a “party” drug sometimes referred to as “ket” or “special K” used at nightclubs, dance parties and raves often in combination with alcohol and other drugs such as cannabis or MDMA. Some of these agents can have an additive effect slowing ketamine metabolism.

Ketamine can be administered by IV or intramuscular injection, nasal, sublingual, or oral routes. It is readily soluble in aqueous solution or lipids and distributes rapidly in tissues. It crosses the blood brain barrier acting on the central nervous system.
Bioavailability is highest by intravenous administration with onset of action within minutes and rapid clearance within about 2 hours. Nasal administration is more variable with slower onset and less control over plasma levels. The graph above demonstrates plasma levels by differing routes of administration.
Metabolism is primarily by the liver and chronic use may be hepatotoxic.
Ketamine is considered to have high abuse potential and can result in addiction. There is a paucity of literature on withdrawal mechanisms however symptoms may include intense craving, insomnia, fatigue, anxiety, and depressive symptoms. Timeline is variable and may last for about three weeks in the acute and subacute phases. Overdose is uncommon and most often results from poly drug use.
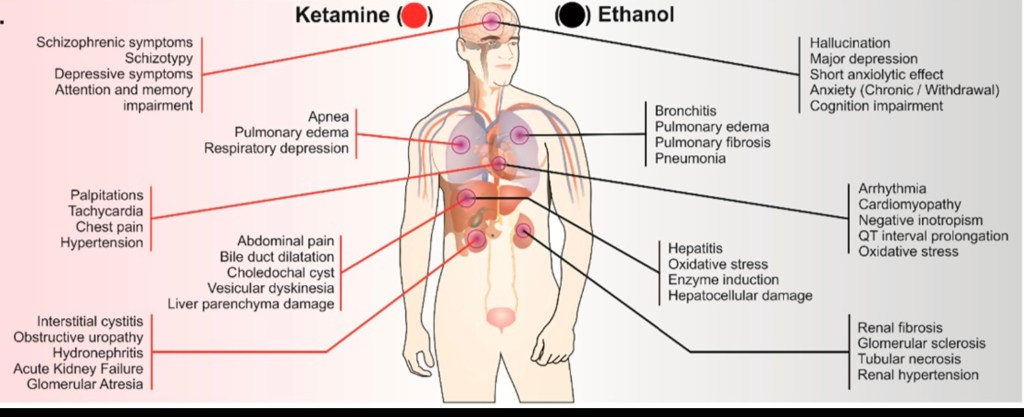
This graphic depicts systemic effects of ketamine and of alcohol as these drugs are commonly used together and can overlap in effects. Ketamine commonly produces upper abdominal pain and may result in liver damage. Cardiovascular effects include rapid heart beat and hypertension. Dizziness, nausea and vomiting may occur.

A potential side effect of chronic ketamine use is damage to the renal collecting system involving the ureters and urinary bladder. The walls of these structures appear to be directly sensitive to the drug resulting in cystic necrotic changes in the lining of these lower urinary structures.
The above CT scans illustrate these effects. On the top left the * star is within a dilated collecting system. On the top right image arrows point to thickened walls of the distal ureters.
In the bottom image white areas represent contrast material excreted from the kidneys. The arrows point to a thickened bladder wall due to ketamine toxicity. The area with the *star toward the bottom of the image is contrast which has collected in the vagina due to a fistula, an abnormal channel connecting the urinary bladder and the vagina due to chronic inflammation. If not dealt with surgically, repeated urinary tract infections will occur.

Ketamine has been found to have a role in treatment of depression, PTSD, suicidal ideation, chronic pain and possibly other indications. These are active areas of investigation. Mechanism of action is incompletely understood however some of the major cellular effects are known.
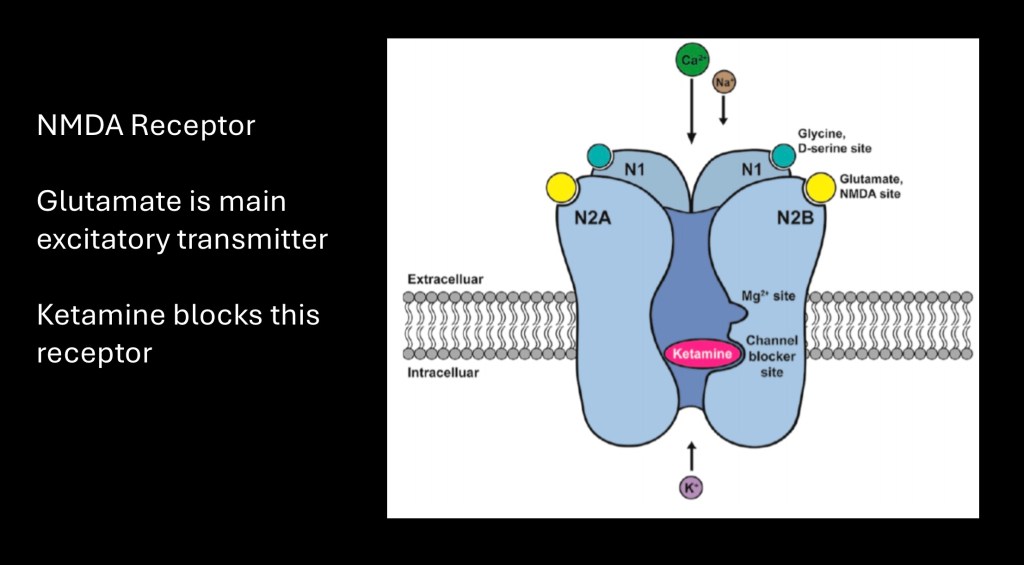
The primary activity of ketamine is as an antagonist, blocking activity of excitatory NMDA glutamate receptors. Glutamate is the most abundant neurotransmitter in the brain. When activated glutamate receptors are excitatory, generating an action potential. There are several types of receptors. Ketamine (red oval) acts on one of these receptor types, NMDA by blocking the central channel and preventing flow of positively charged Ca++ ions.

The precise mechanism by which ketamine can relieve clinical depression by up to several weeks from a single dose is not completely clear. The above diagram illustrates one proposed mechanism.
In addition to NMDA receptors there is a second glutamate receptor type AMPA which is not blocked by ketamine. So when glutamate is released it activates AMPA receptors. Glutamate release is promoted by ketamine effects on nearby GABA receptors. This initiates a cascade of reactions resulting in production of the regulatory protein mTOR causing production of new synapses with adjacent neurons. These new neuroplastic neural pathways are thought to form the basis of clinical response to ketamine in depression. In a real sense ketamine “rewires” your brain.

More detail on the above mechanism and formation of neural circuits following treatment with ketamine. Sites of ketamine action are shown in pink boxes. Glutamate acting on AMPA receptors results in formation of new synapses and antidepressant activity.
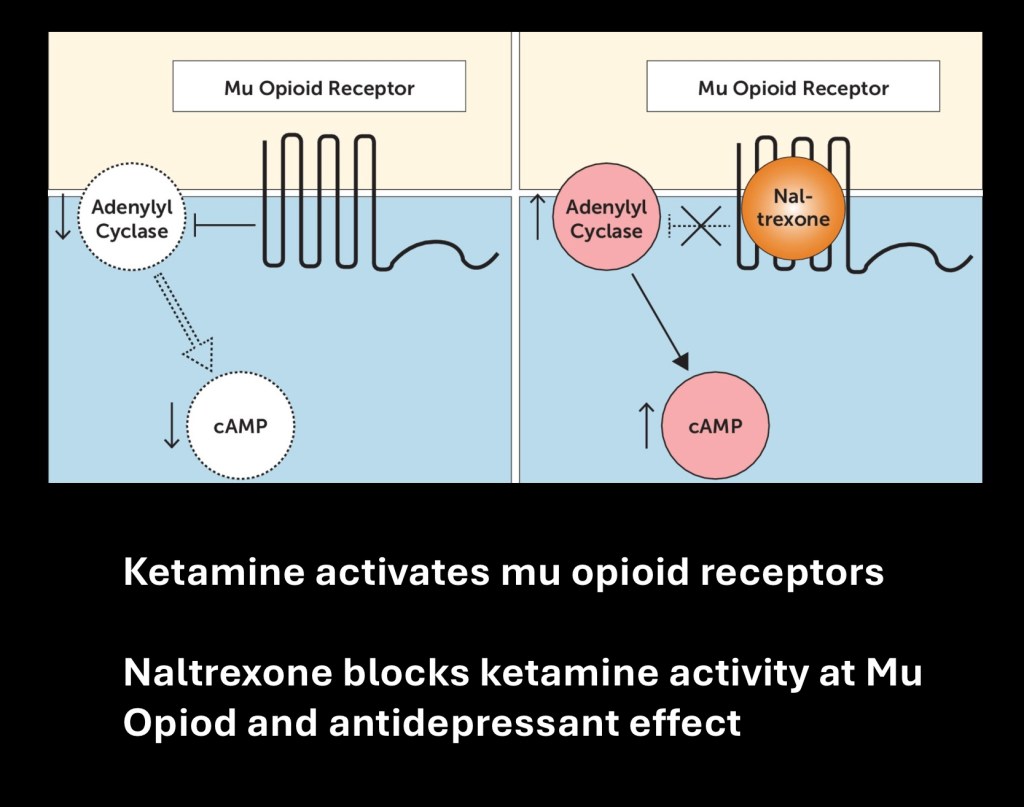
Another site of ketamine action is thought to contribute to antidepressant properties. Ketamine activates mu opioid receptors. In effect it acts similar to morphine. On the right mu opioid receptor activation blocks the chemical signaling pathway shown.
In preclinical animal research when the opiate receptor antagonist naltrexone (Revia) is given prior to a dose of ketamine expected antidepressant effects do not occur. This provides strong evidence that opioid activity of ketamine is integral to its antidepressant effects. This activity is also thought to be responsible for the analgesic and rewarding effects of ketamine.

fMRI studies and preclinical research strongly suggest that the frontal lobe and hippocampus are focused sites of ketamine activity. The frontal lobe is the primary site of cognitive activity, decision making, and emotional regulation. The hippocampus is involved with long term memory and emotional processing.
Ketamine is thought to strengthen neural pathways in brain centers regulating stress response and mood.
The next section looks at some clinical trials using Ketamine.

This study evaluated the effects of ketamine treatment on suicidal ideation. 80 patients with major depression and suicidal ideation were enrolled in the study and randomly assigned to either placebo or IV ketamine infusion at 0.5 mg/kg. Standard antidepressant medication was maintained throughout the study. The short acting benzodiazepine Midazolam (versed) was used as placebo to simulate effects of ketamine. The study was double blinded to subjects and patients.
The graph demonstrates significant reduction in suicidal ideation in the ketamine group (red) as measured by the Scale for Suicidal Ideation (SSI). There was suboptimal reduction at day one in the placebo group (green). The Midazolam placebo group was then switched to ketamine treatment (orange) for ethical reasons due to sub clinical improvement with Midazolam. Both groups remained at low SSI levels with follow up to 6 weeks.

Level of depression measured by the Hamilton Depressive Rating Scale using the same protocol. Greater reduction was seen in the ketamine group (red) than in the placebo group (green) at day one. Switch to ketamine for the placebo group demonstrated significant reduction in depression score (orange).
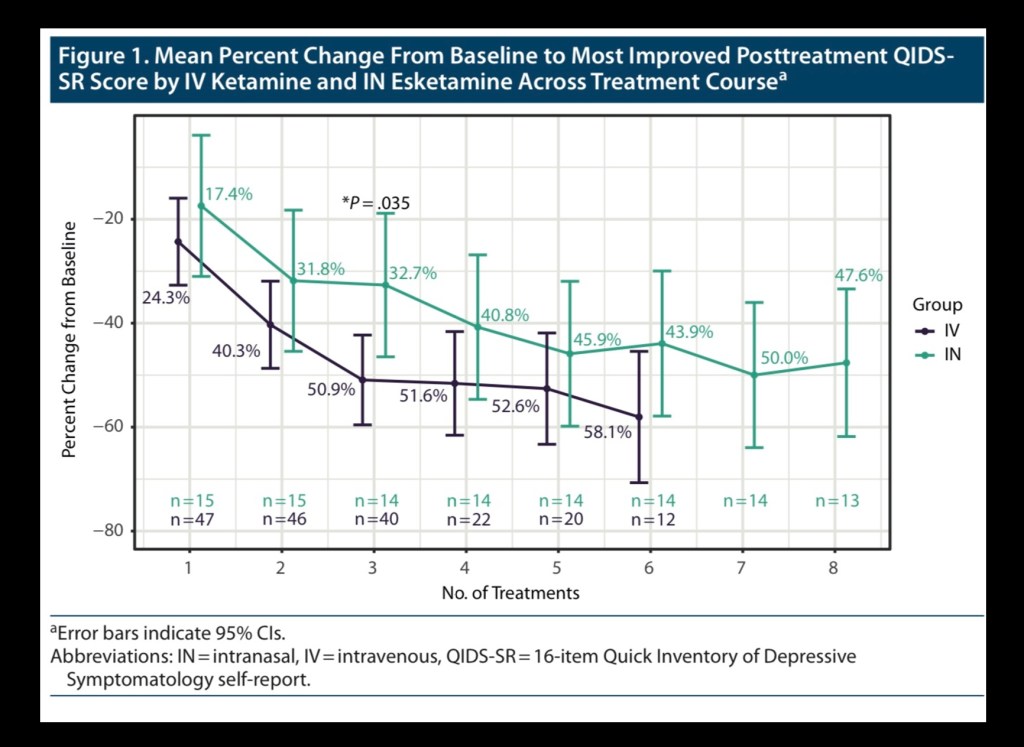
Recently a fixed dose nasal preparation of esketamine (Spravalto) has become available more suited to outpatient and telemedicine therapy. This study compared the nasal preparation with standard IV ketamine in patients with major depression measured by QIDS-SR score. Slightly greater improvement and fewer doses to reach maximal improvement were seen in the IV ketamine group. The results did indicate that intranasal administration is a viable option.

While ketamine has a high safety profile and efficacy it is not a benign drug. Potential for abuse and addiction has been noted. Currently there are a limited number of epidemiology studies related to non medicinal use. Central nervous system and other systemic effects have been discussed above. This graphic describes additional potential side effects associated with ketamine use.

This study from 2011 estimated ketamine use patterns in the US, UK, Australia, and Canada. Rates varied significantly between countries with the lowest rates in the US (0.1%) and the highest rates in the UK (4.0%). Current accurate statistics on non medicinal ketamine use are not readily available.
There have been some case reports and limited studies looking into ketamine as an agent to treat addiction. At this time there is insufficient data to evaluate this drug for treatment of substance use disorder.

Well known actor Mathew Perry who played a leading role as Chandler in the sitcom “friends” and many other roles in TV and movies passed away in October 2023. He was found dead in his hot tub at his Los Angeles home. The coroner ruled his death was due to “acute effects of ketamine” and drowning. He had been receiving ketamine therapy however the large amount present was not consistent with the controlled therapeutic course he had been receiving.
Mathew Perry lived through a long and difficult battle with substance addiction beginning at the age of 14. He shared a detailed account of his struggle with the disease in his best selling book “Friends, Lovers, and the Big Terrible”. He became a philanthropist and advocate for legal reform aimed at increasing opportunities for addiction treatment in his lifetime.
……………………………………………………………
Thank you for your time and effort in reviewing this post. I welcome any feedback or comments.
This post should not be considered medical or professional advice. For information and educational purposes only. Images and data obtained from sources freely available on the World Wide Web.
Jeff K. 3/24
……………………………………………………………………..
References
Ketamine
Ketamine abuse potential and use disorder Yu Liu1, Deyong Lin1, Boliang Wu1, Wenhua Zhou1,2*
1.Laboratory of Behavioral Neuroscience, School of Medicine, Ningbo University, Ningbo 315211, P.R. China
2.Ningbo Addiction Research and Treatment Center,Ningbo 315010, P.R. China
https://www.sciencedirect.com/science/article/abs/pii/S036192301630123X
………………………………………………………………………
Ketamine for the treatment of addiction: evidence and potential mechanisms
Ivan Ezquerra-Romano, I 1; Lawn, W 2, Krupitsky, E. 3, Morgan, CJA 2,4 *
1. Department of Neuroscience, Physiology and Pharmacology, University College London, Gower Street, London, UK
…………………………………………………………………………….
Ketamine Pharmacology: An Update (Pharmacodynamics and Molecular Aspects, Recent Findings)
Georges Mion, Thierry Villevieille
https://onlinelibrary.wiley.com/doi/full/10.1111/cns.12099
………………………………………………………….
The Neurobehavioral Pharmacology of Ketamine: Implications for Drug Abuse, Addiction, and Psychiatric Disorders
Keith A. Trujillo, Monique L. Smith, Brian Sullivan, Colleen Y. Heller, Cynthia Garcia,
………………………………………………………………….
Ketamine Psychedelic Psychotherapy: Focus on its Pharmacology, Phenomenology, and Clinical Applications
Eli Kolp
Private Practice, Sarasota, FL
Harris L. Friedman University of Florida
Evgeny Krupitsky
St. Petersburg State Pavlov Medical University
………………………………………………………
https://academic.oup.com/pmj/article/90/1062/185/6992068
Evaluation of the extent of ketamine-induced uropathy: the role of CT urography
Li-Kuo Huang, Jia-Hwia Wang, Shu-Huei Shen, Alex T L Lin, Cheng-Yen Chang
Postgraduate Medical Journal, Volume 90, Issue 1062, April 2014, Pages 185–190,
………………………………………………………….
Assessment of ketamine uropathy
Author links open overlay panel
Stephen S. Yang a, Chun-Hsien Wu b, Judy Yi-Ju Chen a c, Shang-Jen Chang a
Team for National Registration of Ketamine Uropathyx
https://www.sciencedirect.com/science/article/pii/S1879522615004261
……………………………………………………
Ketamine for Depression: Where Do We Go from Here?
Marije aan het Rot, Carlos A. Zarate Jr., Dennis S. Charney, and Sanjay J. Mathew Department of Psychology and School of Behavioral and Cognitive Neuroscience (MahR), University of Groningen, The Netherlands; Experimental Therapeutics and Pathophysiology
Biol Psychiatry. 2012 October 1; 72(7): 537–547. doi:10.1016/j.biopsych.2012.05.003.
………………………………………………………
……………………………………………………..
Mechanisms of Ketamine Action as an Antidepressant
Panos Zanos, Ph.D.a,* and Todd D. Gould, M.D.a,b,c
aDepartment of Psychiatry, University of Maryland School of Medicine, Baltimore,
Mol Psychiatry. 2018 April ; 23(4): 801–811. doi:10.1038/mp.2017.255.
…………………………………………………………
Ketamine plus Alcohol: What We Know and What We Can Expect about This
Natalia Harumi Correa Kobayashi 1,†, Sarah Viana Farias 1,†, Diandra Araújo Luz
Kissila Márvia Machado-Ferraro 1, Brenda Costa da Conceição 1, Cinthia Cristina Menezes
Int. J. Mol. Sci. 2022, 23, 7800. https://doi.org/10.3390/ijms23147800
……………………………………………………………..
To use or not to use: an update on licit and illicit ketamine use
Review
Substance Abuse and Rehabilitation 2011:2 11–20
© 2011 Li et al, publisher and licensee Dove Medical
………………………………………………………..
An Investigation to Dissociate the Analgesic and Anesthetic Properties of Ketamine Using Functional Magnetic Resonance Imaging
Richard Rogers, M.B.B.S., F.R.C.A.; Richard G. Wise, Ph.D.; Deborah J. Painter, M.B.Ch.B., F.R.C.A.; Sarah E. Longe, M.Sc.; Irene Tracey, D.Phil.
Author and Article Information
Anesthesiology February 2004, Vol. 100, 292–301.
………………………………………………………………….
Effect of Ketamine on Limbic GABA and Glutamate: A Human In Vivo Multivoxel Magnetic Resonance Spectroscopy Study
Front. Psychiatry, 07 September 2020
Sec. Mood Disorders
Volume 11 – 2020 | https://doi.org/10.3389/fpsyt.2020.549903
https://www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2020.549903/full
…………………………………………………………………..
https://www.nature.com/articles/s41380-024-02419-6
……………………………………………………………….
Ketamine for depression Luke A. Jelen & James M. Stone
To cite this article: Luke A. Jelen & James M. Stone (2021): Ketamine for depression, International Review of Psychiatry
To link to this article: https://doi.org/10.1080/09540261.2020.1854194
………………………………………………………………
Ketamine for depression: evidence, challenges
and promise
CARLOS A. ZARATE JR., MARK J. NICIU
Experimental Therapeutics and Pathophysiology Branch, National Institute of Mental Health, National Institutes of Health, Bethesda, MD
……………………………………………………………….
Antidepressant Effects of Ketamine in Depressed Patients
Robert M. Berman, Angela Cappiello, Amit Anand, Dan A. Oren,
2000 Society of Biological Psychiatry
…………………………………………………………………..
Oral Ketamine for Depression, 2: Practical Considerations
Chittaranjan Andrade, MD
Published: April 9, 2019
The Journal of
• Clinical Psychiatry
………………………………………………………………………
Ketamine: 50 Years of Modulating the Mind
Front. Hum. Neurosci., 29 November 2016
Sec. Brain Health and Clinical Neuroscience
Volume 10 – 2016 | https://doi.org/10.3389/fnhum.2016.00612
https://www.frontiersin.org/articles/10.3389/fnhum.2016.00612/full
………………………………………………
Ketamine beyond anesthesia: Antidepressant effects and abuse potential
Keith A. Trujillo*,
Department of Psychology and Office for Training, Research, and Education in the Sciences, California State University San Marcos, 333 S. Twin Oaks Valley Road, San Marcos, CA, 92096, United States
Sergio D. Iñiguez
Department of Psychology, The University of Texas at El Paso,
Behav Brain Res. 2020 September 15; 394: 112841. doi:10.1016/j.bbr.2020.112841.
………………………………………………….
Rapid neuroplasticity changes and response to intravenous ketamine: a randomized controlled trial in treatment-resistant depression
- Jared Kopelman,
https://www.nature.com/articles/s41398-023-02451-0
……………………………………………………….
Role of the AMPA receptor in antidepressant effects of ketamine and potential of AMPA receptor potentiators as a novel antidepressant
Neuropharmacology January 2023, 109308
https://www.sciencedirect.com/science/article/pii/S0028390822003677
…………………………………………………………
Treatments
……………………………………………………………
Ketamine for Rapid Reduction of Suicidal Thoughts in Major Depression: A Midazolam-Controlled Randomized Clinical Trial
Michael F. Grunebaum, M.D., Hanga C. Galfalvy, Ph.D., Tse-Hwei Choo, M.P.H., John G. Keilp, Ph.D., Vivek K. Moitra,
Published Online:5 Dec 2017https://doi.org/10.1176/appi.ajp.2017.17060647
https://ajp.psychiatryonline.org/doi/full/10.1176/appi.ajp.2017.17060647
…………………………………………………………….
The epidemiology and patterns of acute and chronic toxicity associated with recreational ketamine use
Sarbjeet S. Kalsi1,2, David M. Wood2,3,4 and Paul I. Dargan2,3,4*
1Emergency Department, Guy’s and St Thomas’ NHS Foundation Trust, London, UK; 2Clinical Toxicology,
https://www.tandfonline.com/doi/pdf/10.3402/ehtj.v4i0.7107
……………………………………………………………….
Dual action of ketamine confines addiction liability
https://doi.org/10.1038/s41586-022-04993-7 Received: 10 December 2021
Accepted: 17 June 2022
Published online: 27 July 2022
Nature | Vol608 | 11August2022
Linda D. Simmler1,3, Yue Li1,3, Lotfi C. Hadjas1, Agnès Hiver1, Ruud van Zessen1

Leave a comment