

Pharmacology and
CNS effects
Ethanol is the oldest known and most widely used psychoactive drug in history. The United States has one of the highest rates of alcohol use in the world. 2019 data report that 69% of adults had used alcohol in the past year. In the same year an estimated 14 million people were affected with Alcohol Use Disorder (AUD) in the US. Total economic cost for misuse of alcohol in 2010 was $245 billion dollars. 29% of deaths from motor vehicle accidents have been attributed to alcohol use in the US. It is estimated that AUD accounts for 6% of global deaths.
This post looks at the pharmacology of ethanol and some of the central nervous system effects of acute and chronic alcohol use. Despite the widespread usage and long history of alcohol much of the biological effects of this drug are still poorly understood. Differing from other psychoactive substances ethanol quickly distributes throughout the brain affecting multiple cellular mechanisms with overlapping effects.
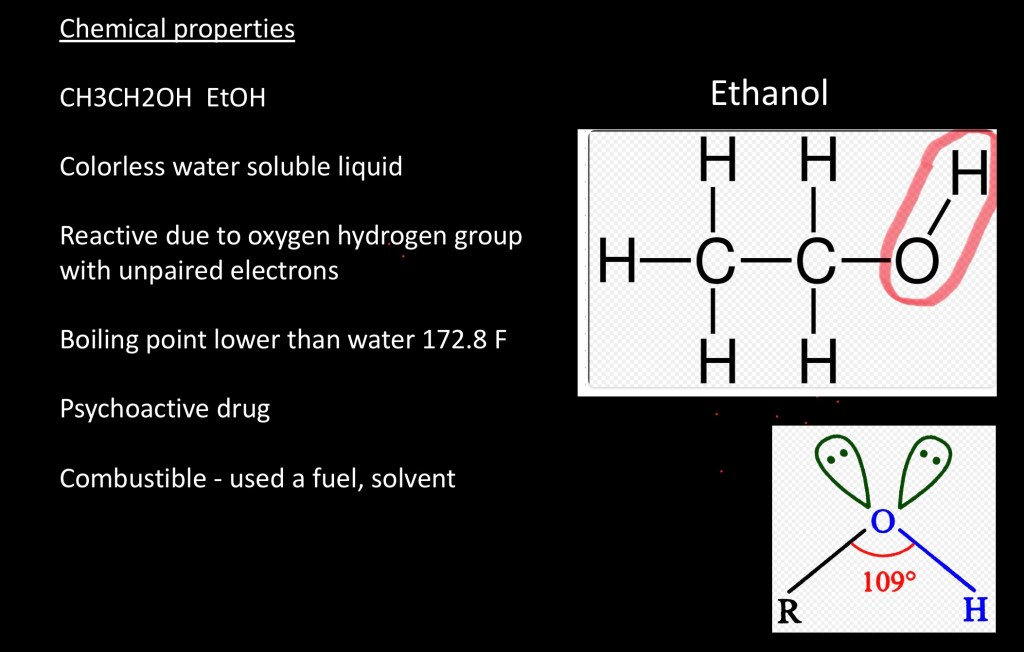
Ethanol (EtOH) is a short chain alcohol composed of a saturated two carbon chain and a Hydroxy (-OH) group. It is a water soluble, colorless liquid with a distinctive odor. Chemical reactivity is due to the presence of unpaired electrons in the oxygen atom allowing for electron transfer and bond formation. Ethanol is combustible and it is used as fuel commonly found as a gasoline additive. It is also used as a solvent and an antiseptic. In the past it was often used for medical anesthesia. It is readily produced from a number of naturally occurring plant sources.
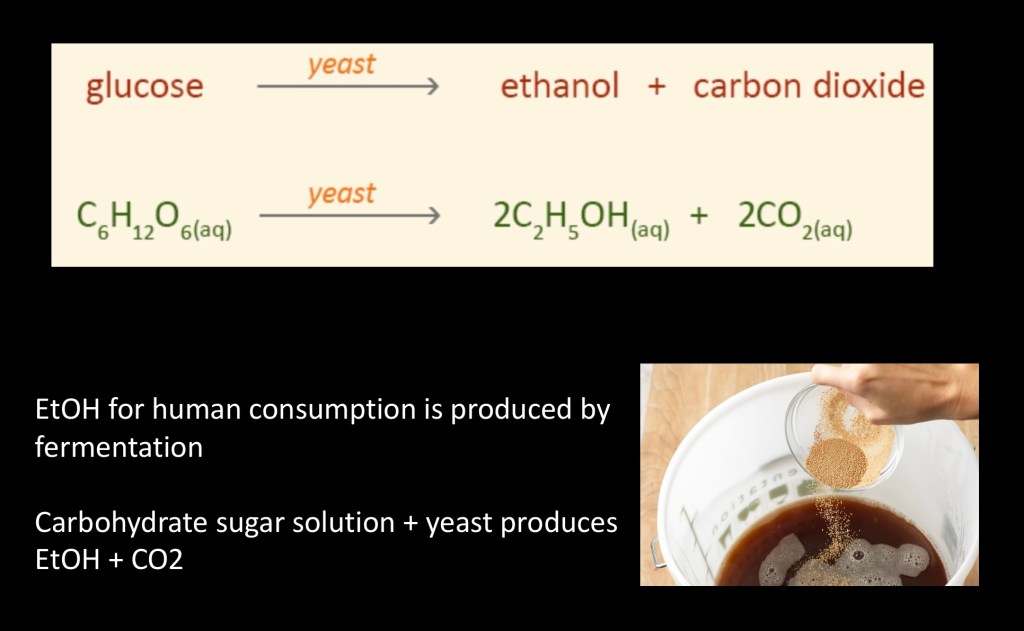
Ethanol for human consumption is produced by fermentation. The process involves addition of yeast species to a solution containing sugars or complex carbohydrates. The yeast breaks down sugars into ethanol and carbon dioxide. Various high carbohydrate substances can be used as a base such as corn, malt, potatoes, grains, grapes and other fruits. There are other synthetic reactions used for industrial production of ethanol and other alcohols.
By this method alcohol concentrations of up to 18% can be obtained. Above this level alcohol concentrations destroy the yeast ending the reaction.
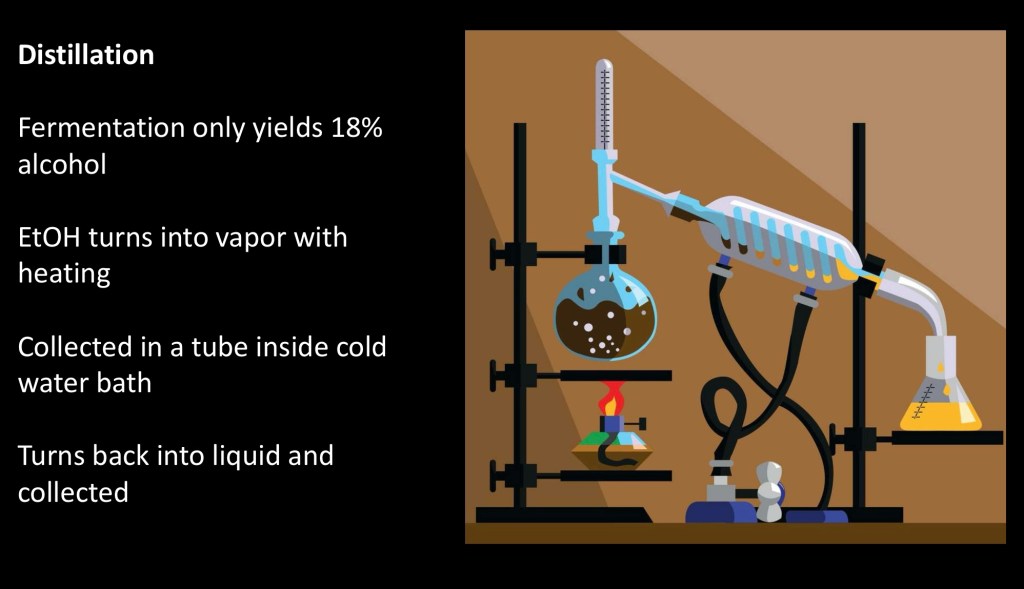
Distillation is used to further concentrate alcohol content in aqueous solutions. The process takes advantage of the lower boiling point of alcohol compared to water.
- The fermented mixture is heated allowing ethanol vapor to rise up the column.
- Ethanol vapor passes through a downward slanting tube encased in a cold water bath.
- This allows the vapor to condense back to a liquid and to be collected in a receiving vessel.
- The process can be repeated to obtain higher concentrations and purity.
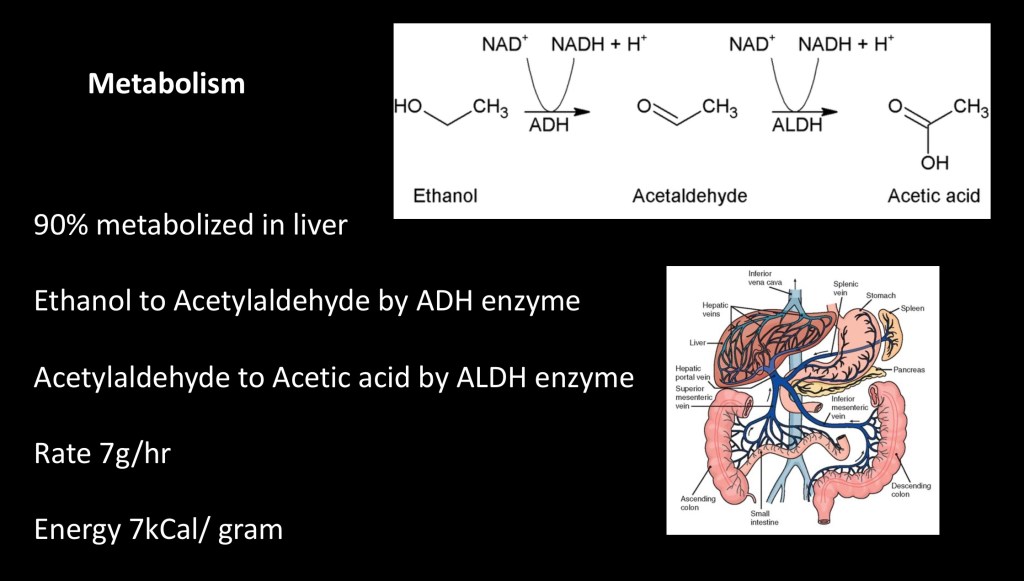
Metabolism breaks down alcohol by a two step process, first to Acetylaldehyde and then to acetic acid (vinegar). The first step is catalyzed by the enzyme alcohol dehydrogenase (ADH). The second step is catalyzed by aldehyde dehydrogenase (ALDH). Acetate is then absorbed into the circulating bloodstream and is further processed in tissues by the citric acid cycle into energy (ATP).
90% of ethanol metabolism occurs in the liver. Alcohol is readily absorbed by the small intestine entering the portal system to the liver and then into the circulating bloodstream. Following ingestion a variable fraction is processed in the stomach by gastric ADH. Remaining non metabolized alcohol exits unchanged through the lungs or kidneys.
There are genetic variants of the ADH and ALDH enzymes. People with the less efficient ALDH2 variant allele experience a buildup of Acetylaldehyde resulting in a “flush” and unpleasant sensations. Faster alcohol metabolism resulting in more rapid clearance due to the ADH1c and ADH1b alleles has been associated with lower risk of alcohol dependence.
Metabolic rate is highly variable. Differences in body fat/water composition, rate of ingestion, sex (M>F) and liver function contribute to alcohol clearance. Approximately 7g/hr can be processed on average. Energy gain is approximately 7kcal/gm. By comparison fat yields 9kcal/gm, and protein 4kcal/gm. A standard US drink is around 14 gm of alcohol.
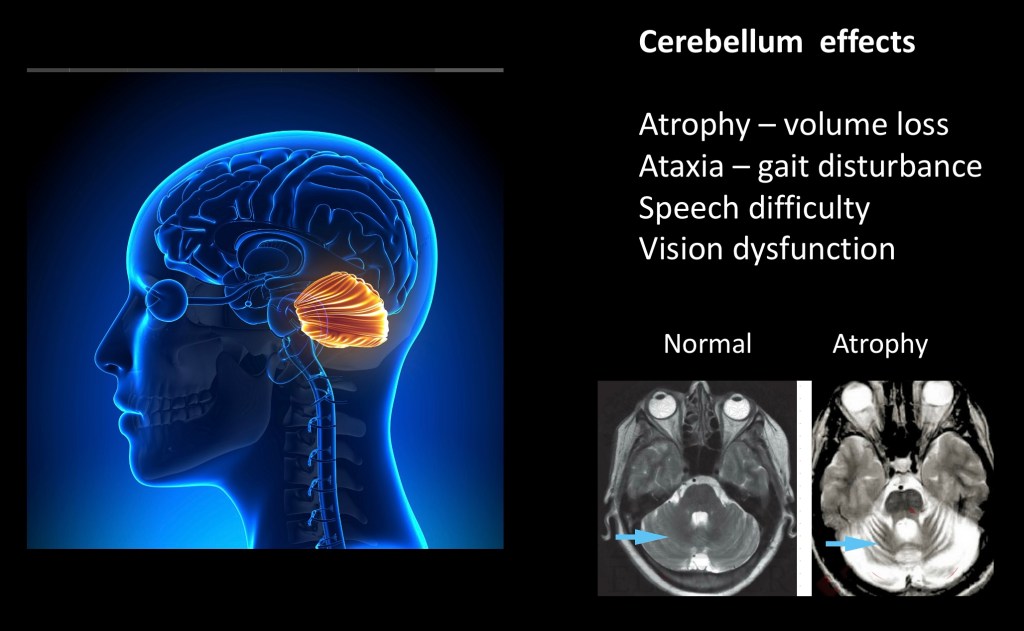
The cerebellum is located at the posterior floor of the brain. The cerebellum is particularly susceptible to both acute and chronic effects of alcohol. It is where neuromuscular coordination is processed, receiving sensory inputs and sending afferent information to coordinate movement. Although it comprises only 10% of brain by volume it contains around 80% of total neurons in the brain.
Functional acute and chronic cerebellar changes include gait abnormalities (ataxia) muscular incoordination (tremor), speech abnormalities (dysarthria), and ocular motor dysfunction (nystagmus).
The MRI above demonstrates cerebellar atrophy. In this T2 weighted sequence fluid is bright. Arrow points to cerebellar tissue decreased in size in comparison to normal. Atrophy represents permanent tissue loss.
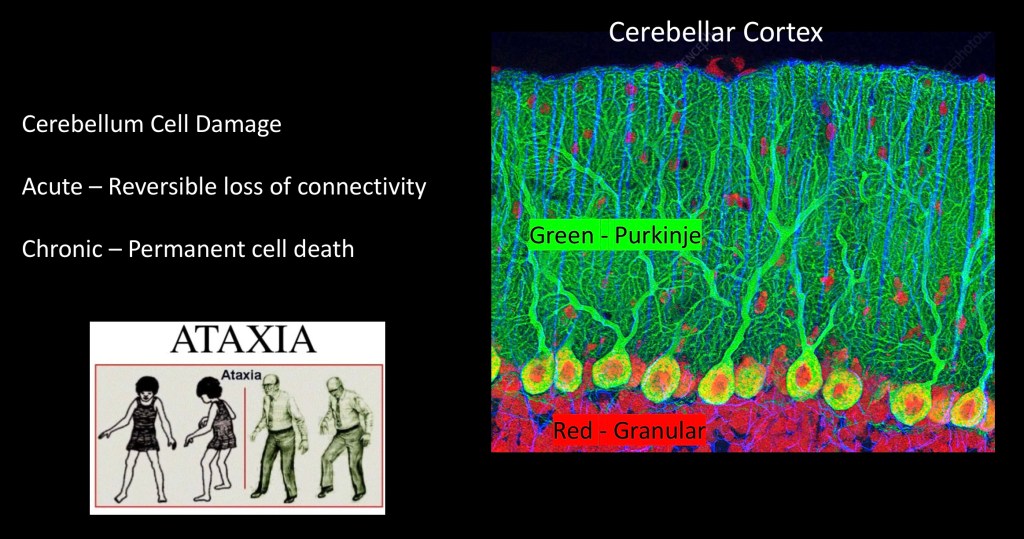
Acute alcohol intoxication results in staggering gait differentiating it from the compensatory widening ataxia seen in chronic alcoholism. Shown above in green is the outermost layer consisting of purkinje cells. These carry signal out of the cerebellum to the periphery. The next deeper layer of cells shown in red are the granular cells which process input signals and then synapse with cortical purkinje cells.
Acute intoxication interferes with synaptic transmission between these cell layers. Ethanol inactivates sodium – potassium ion pumps decreasing cellular activity. It also activates inhibitory GABA receptors located in the granular cell layer. Gait abnormality results from slower communication and decreased activity of cerebellar function necessary to coordinate lower extremity movement.
Acute changes are reversible following discontinuation of the substance.
Chronic exposure can lead to cellular necrosis and brain atrophy. Alcohol is toxic to mitochondria resulting in generation of oxidation free radicals and decrease of cellular energy production. This process induces irreversible functional brain abnormalities
Classic cerebellar findings include a widened stance, slow speed and short strides when walking. Lower and upper extremity tremors may be present. Consumption of 150g alcohol daily for 10 years has been shown to result in chronic cerebellar abnormalities in 30% of patients.
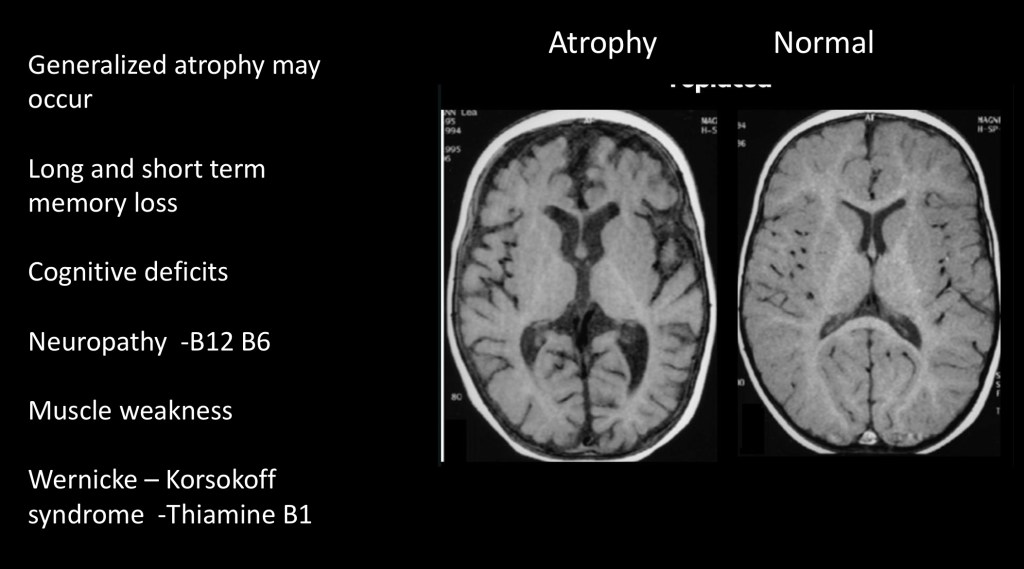
Atrophy with loss of brain tissue is not limited to the cerebellum and may be seen throughout the brain. The frontal lobes are most vulnerable to cell damage resulting from chronic alcohol use. Oxidative stress plays a key role in cell death. In addition there is often demyelination of white matter tracts resulting in slower inefficient cellular communication.
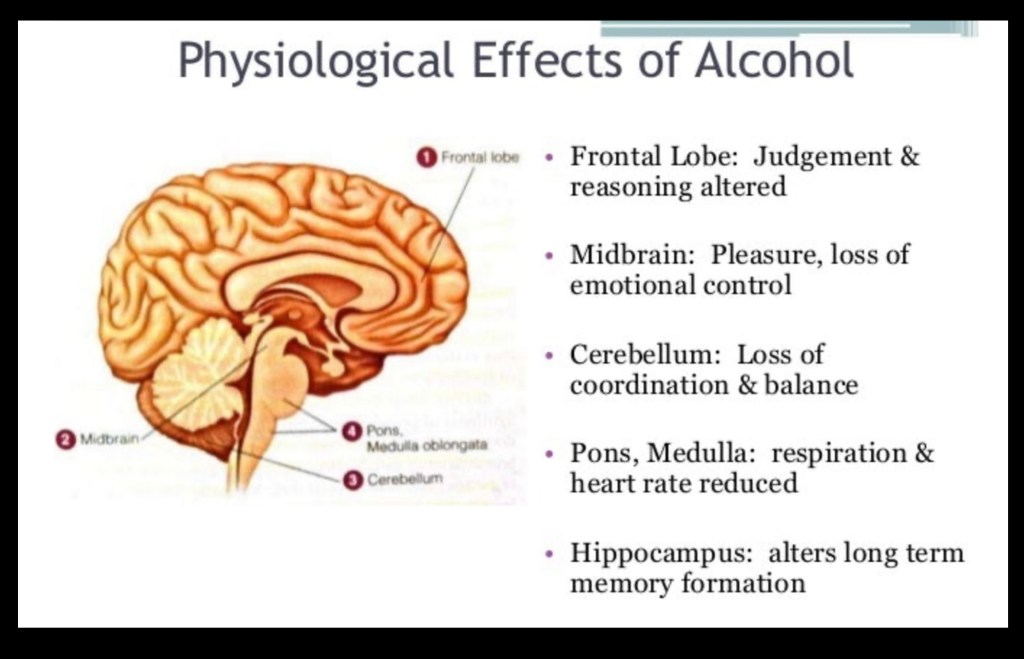
The above diagram summarizes physiologic effects of alcohol and brain structures involved. In addition to the cerebellum the frontal lobes, the hippocampus, midbrain and pons are affected which can result in significant neurologic deficits.
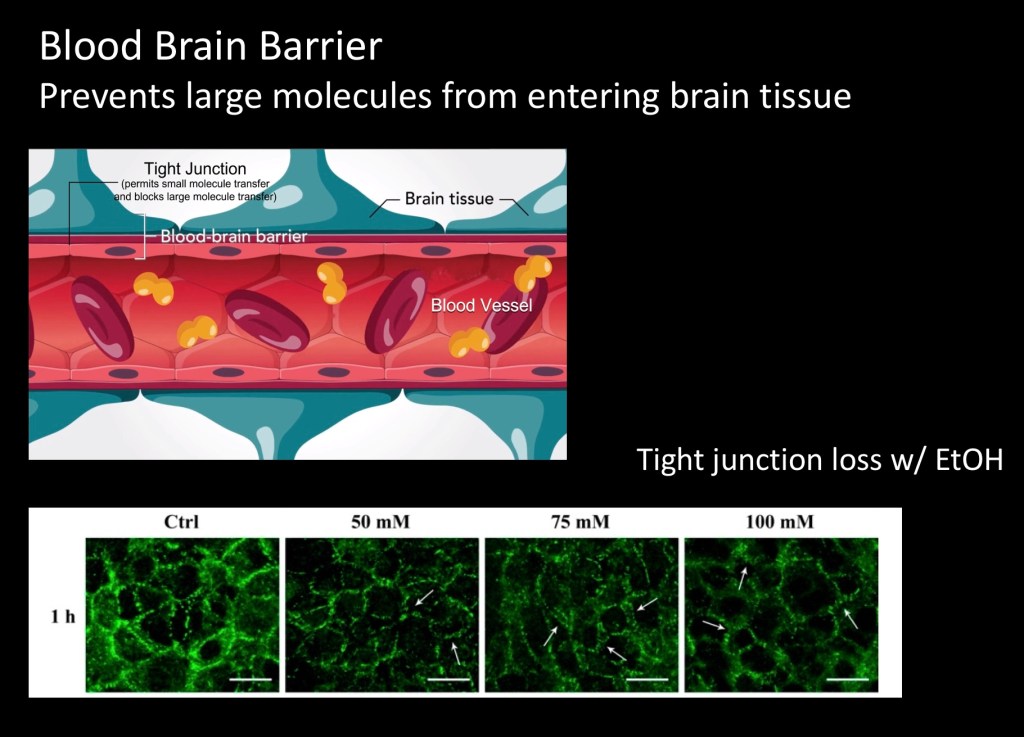
The blood – brain barrier is an essential property of blood supply to the brain. Blood vessels supplying the brain are surrounded by astrocyte cells and tight junction proteins. These form a barrier selectively blocking some substances from entering the brain and affecting neural function.
Alcohol interferes with the barrier by degrading tight junctions. This results in “leaky” vessels allowing substances to pass through resulting in oxidative stress and inflammation.
The green images above represent tight junction proteins exposed to increasing amounts of ethanol resulting in gaps and thinning of the barrier.
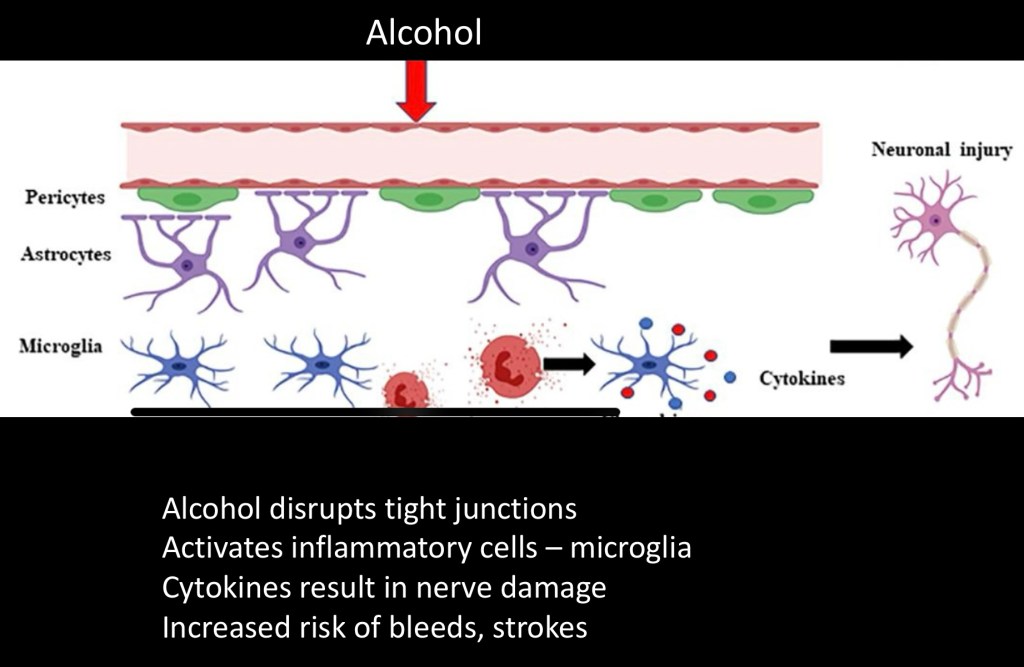
Damage to the blood brain barrier sets up inflammatory reactions with activation of microglia. These are like the white blood cells of the brain. Release of inflammatory cytokines result in further damage to brain tissue with tissue loss.
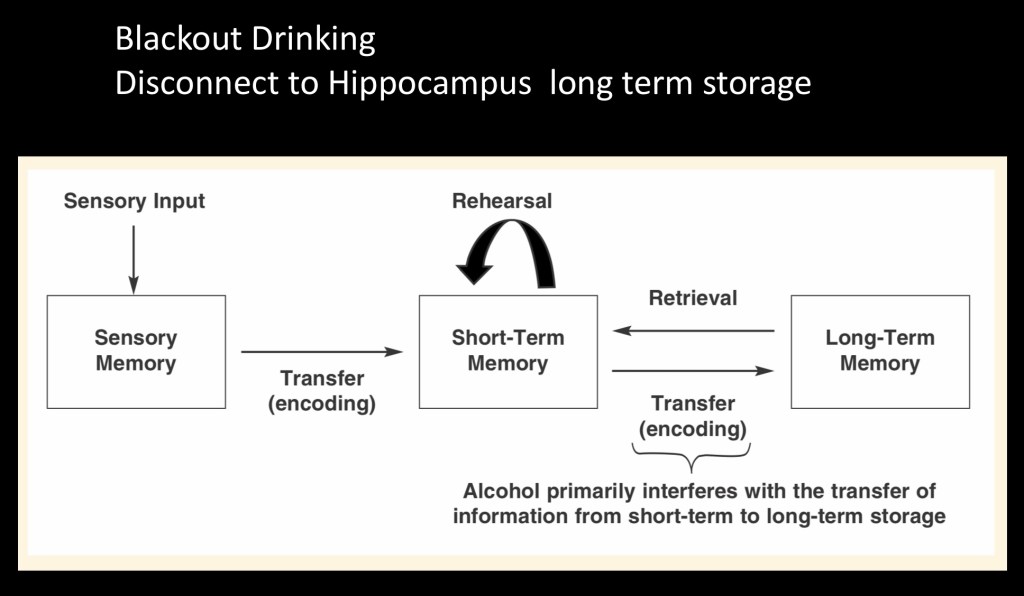
Large doses of ethanol may result in periods of amnesia. During these episodes immediate working memory and short term memory are largely intact. The deficit occurs in lack of storage of long term memory in the hippocampus.
For example intoxicated individuals have been shown to retain paired association in short term recall. The letter B paired with ice cream for example. However they could not remember the association hours later. People in this state are able to carry on conversations and most tasks but have no recollection of large blocks of time later.
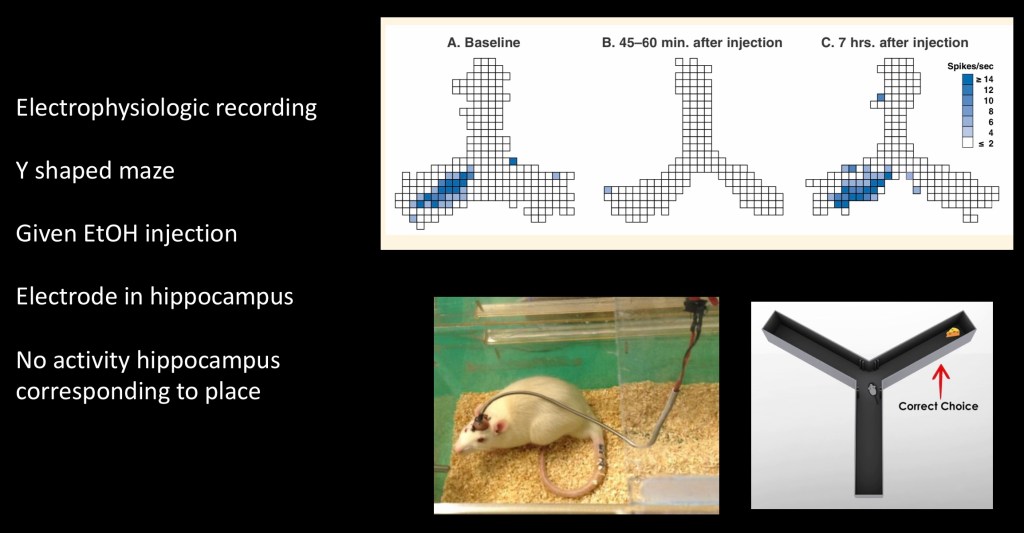
In this experiment localization of memory formation in rats was demonstrated. A tiny microelectrode was placed into the hippocampus. A signal was recorded corresponding to movement into a specific place in the Y shaped maze as shown by blue squares on the left.
In the center map no signals were generated after alcohol injection when the rats were in the same space remembered previously. Following a delay memory signals were again generated by the same animal as shown on the right.
Blackouts result from inhibition of inter neurons to the hippocampus due to increased GABA activity induced by alcohol.
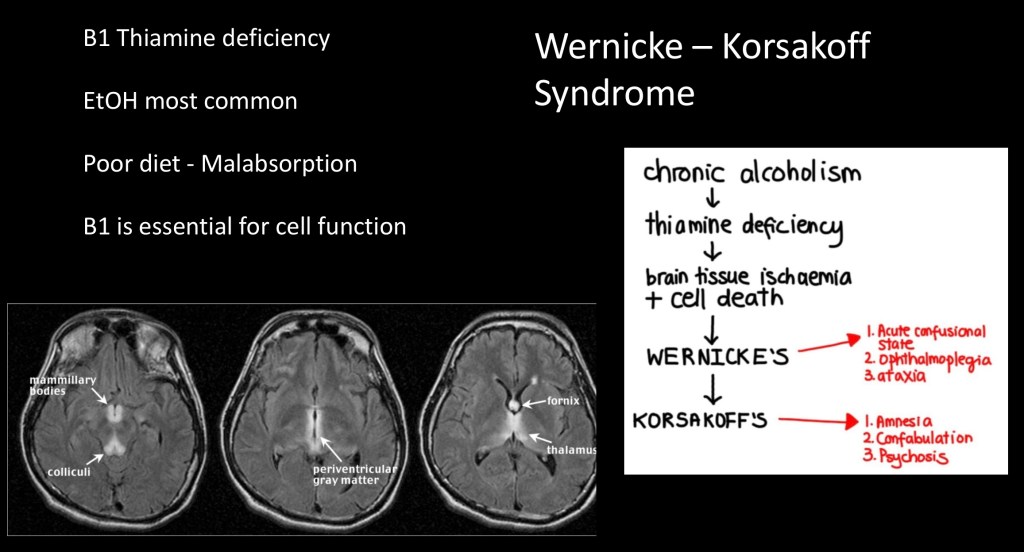
Vitamins are essential substances which we cannot manufacture and must be obtained from dietary sources. Thiamine, vitamin B, is normally found in whole grains and legumes. Processing in western diets removes much of the thiamine content. For this reason it is often added as a supplement in grain based products. Thiamine is needed for the breakdown of glucose and amino acids into energy.
Chronic alcohol users are prone to thiamine deficiency due to poor diet and decreased absorption secondary to alcohol use. This may result in Wernicke and Korsakoff syndromes. It is characterized by a wide ataxic gait, mental confusion, and abnormal eye movements. It may progress to permanent cognitive and memory deficits.
Treatment is recommended as soon as symptoms are suspected preferably with IV thiamine. The MRI above shows typical imaging findings with bright T2 signal in affected deep brain structures.
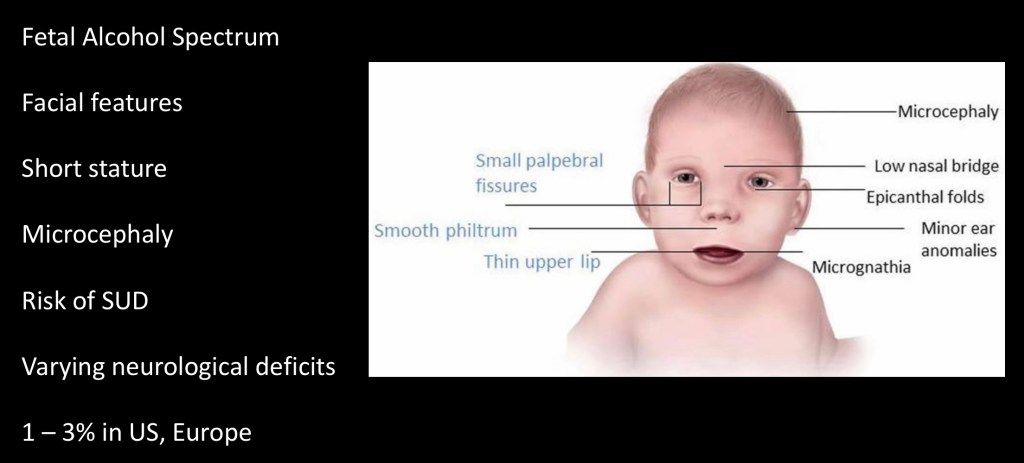
Fetal alcohol spectrum results from alcohol ingestion during pregnancy. Typical facial characteristics are shown above. Most individuals have short stature. Neurologic deficits range from minimal to profound. The spectrum of disorder may include difficulty learning, short attention span, small head size (Microcephaly) and difficulty with coordination. The precise mechanism resulting in the syndrome is unknown at this time.
Actors Jim Carrey and Daniel Radcliffe (Harry Potter) were born with fetal alcohol syndrome and have been advocates raising awareness about the disease.
Mechanism of action within the central nervous system had been thought to be nonspecific acting on membrane ion channels and receptors globally. However more specific activity accounting for much of acute and chronic malfunction has more recently been described.
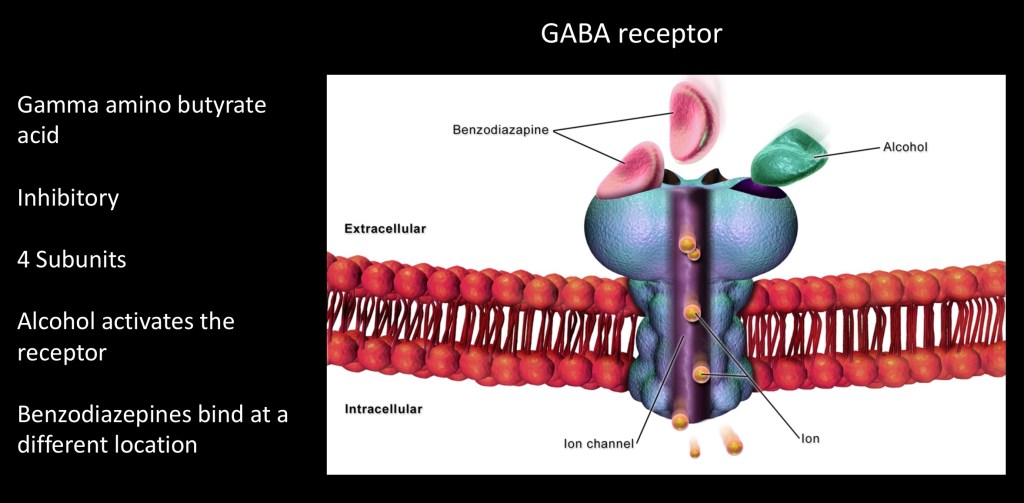
Gamma amino butyric acid (GABA) is the most common inhibitory neurotransmitter in the brain. It has a widespread distribution. GABA is essential to balance and control excitatory signals from glutamate neurons.
There are two types of GABA receptor subunits, types A and B. Each is composed of four subunits. Ethanol acts on the GABAa receptor increasing the effect of the activated neuron. It can also cause increased GABA release by GABAergic neurons. The result is increased inhibition of key neural pathways.
Chronic exposure results in compensatory down regulation of GABA expressing genes in an attempt to rebalance. This affects both early and late withdrawal symptoms.
Benzodiazepines act in a similar manner potentiating GABA signal although on a different binding site. This explains why benzodiazepines are synergistic with alcohol and the combination carries risk of overdose. It also explains why they are useful for EtOH withdrawal.
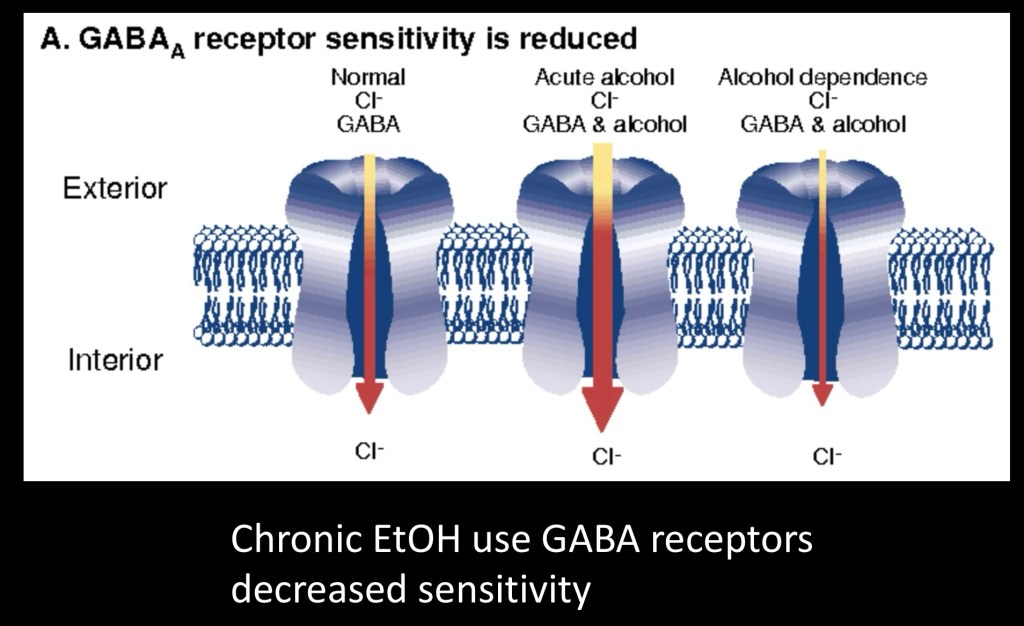
This diagram illustrates how GABA receptors change over time with chronic alcohol use. In acute intoxication the receptors become hyper reactive allowing in more negatively charged Cl- ions decreasing cell activity. Over time the receptor changes configuration becoming less active. This helps to compensate increased GABA transmitter release due to alcohol and the system is partially compensated.
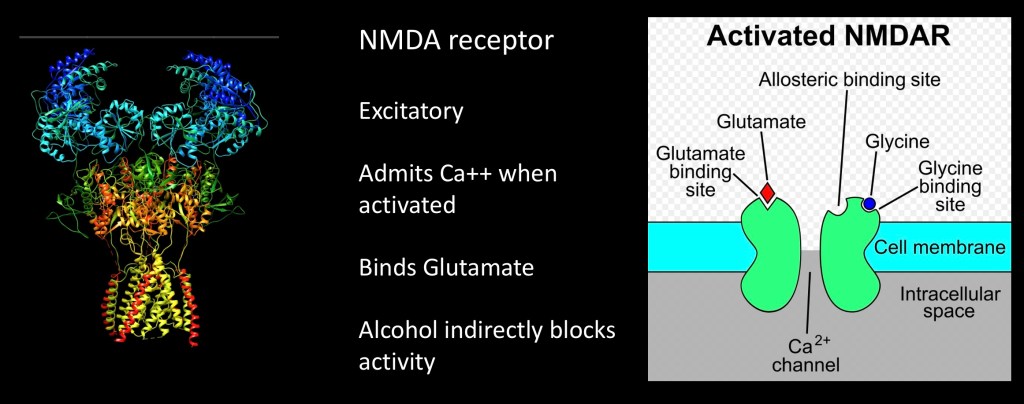
There is another major neurotransmitter affected by alcohol. Glutamine is an excitatory transmitter and the most abundant in the human brain. Shown here is an NMDA glutamine receptor. The structure and function of this receptor is complex with multiple subunits. To activate it must bind a glycine molecule as well as a glutamate molecule. When that happens Calcium Ca++ enters the cell. It activates ion channels downstream and the cell fires. Alcohol interferes with glutamate binding inhibiting excitatory activity.
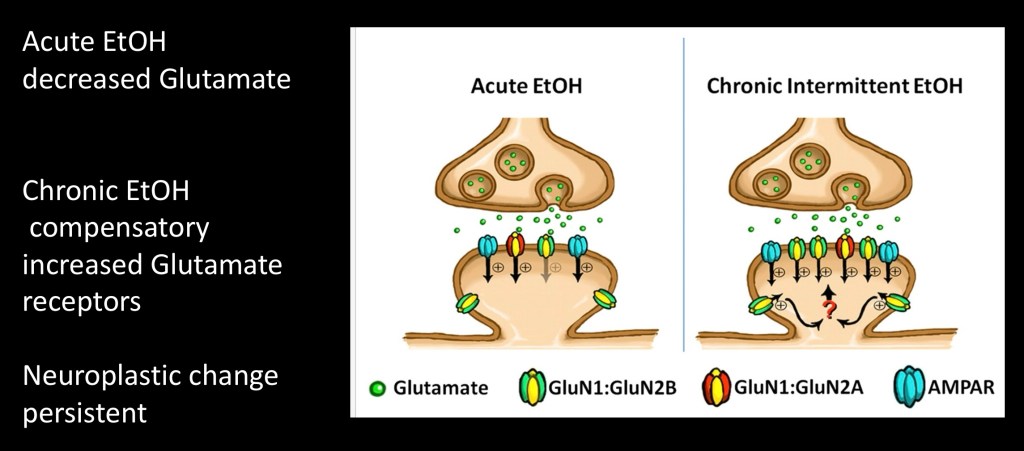
In chronic EtOH use a neuroplastic change occurs in gene expression generating more NMDA receptors to compensate for decreased activity due to alcohol This helps to rebalance the system. These are shown here in green and yellow on the receiving post synaptic membrane. The specific subtype is indicated as GluN1:GluN2b. AMPAR indicates the gated ion channel activated downstream.
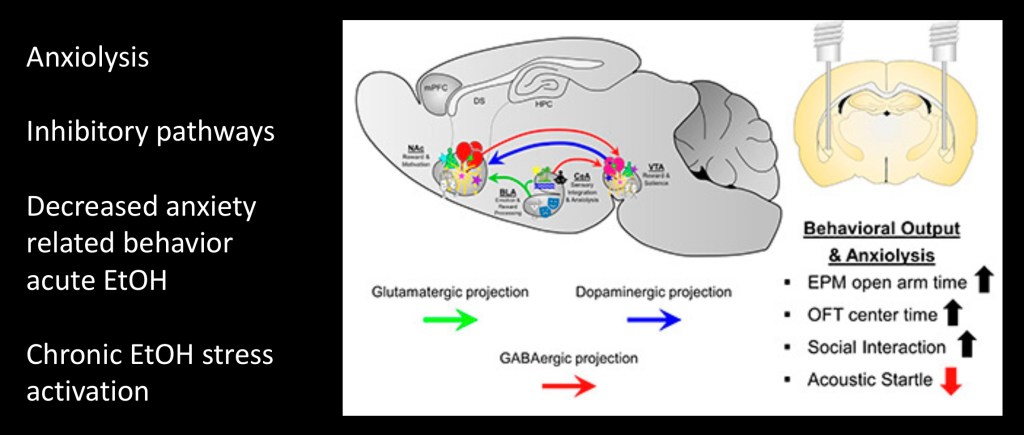
This is a diagram of a mouse brain showing pathways activated by acute alcohol. Dopamine, GABA and Glutamate projections are shown. The effect is to increase dopamine and excitatory signaling to the Nucleus Accumbens a center important in motivation and behavior. There is also decreased activity in the core of the Amygdyla with less anxiety reaction.
In the bottom right corner behavioral correlates present with alcohol administration are listed with decreased anxiety type behaviors and more social behaviors. Addiction is partially driven by a higher baseline stress reaction temporarily relieved by using more alcohol.
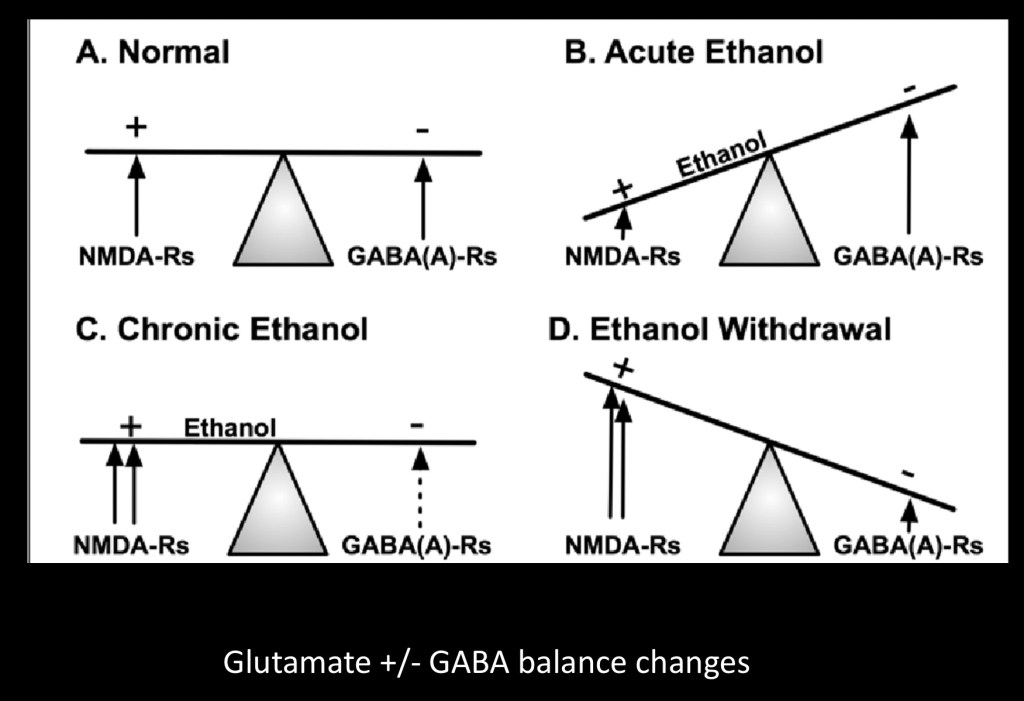
GABA inhibitory and Glutamate excitatory NMDA activity at rest are in balance.
- Normal state enables normal functional responses to environmental change.
- Acute alcohol decreases excitatory and increases inhibitory signals with typical intoxication response
- Chronic alcohol. Compensatory changes rebalance the system when alcohol is in the system
- Withdrawal. Without alcohol the system is out of balance and now there is too much excitatory signal and stress anxiety reaction.
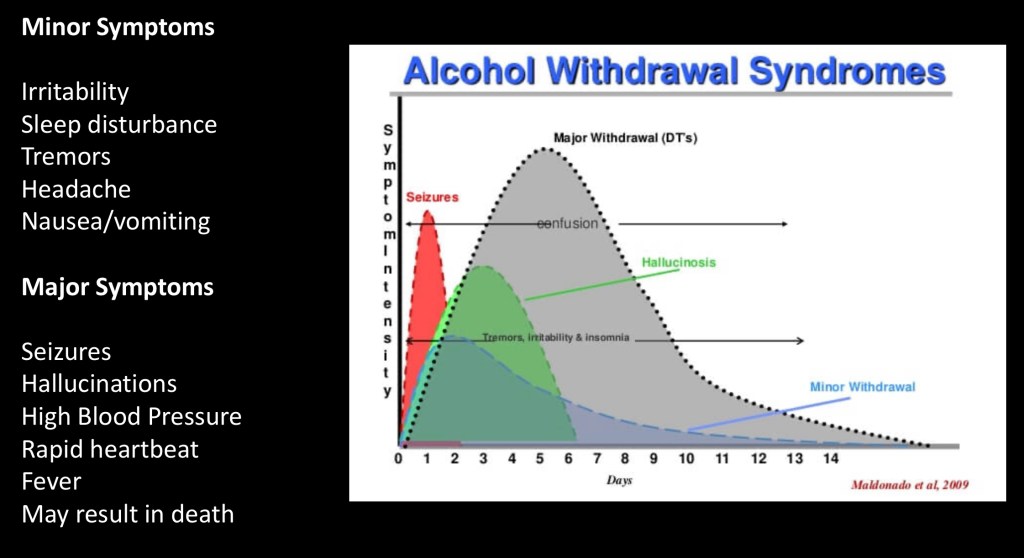
Time activity curves above represent the range of alcohol withdrawal symptoms which can be among the most serious of drug withdrawals.
Minor symptoms include irritability, nausea/ vomiting and sleep disturbance. Major symptoms can include seizures, rapid heartbeat, hallucinations and high blood pressure. Death may occur in about 5% of hospitalized patients and up to 20% without treatment.
Treatment includes benzodiazepines and supportive care, phenobarbital may be given for severe cases. More severe cases often present with multiple medical problems including liver and kidney abnormalities, metabolic, nutritional, and other issues. A multi point scale has been developed CIWA-Ar to aid in clinical management and to gauge need for hospital admission vs outpatient management.
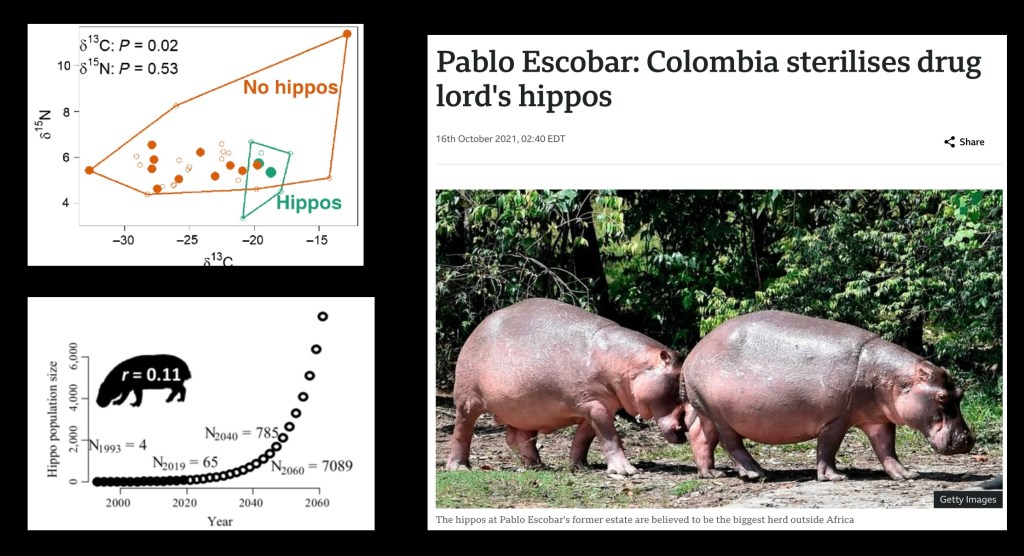
The late Pablo Escobar the former Colombian drug kingpin was an avid collector of exotic animals including this pair of African hippos. His estate was abandoned after his death. The hippos have since become a huge problem and are reproducing and thriving as shown in a scientific study of the matter commissioned by the Colombian government.
Thus far the hippos remain at large as the authorities have dismissed the hippopotamus issue as “simply preposterous”
…………………………………………………………………….
This post is a brief review of ethanol as a psychoactive drug and changes within the central nervous system with acute and chronic use. The cerebellum is a brain structure susceptible to alcohol effects resulting in gait abnormalities and tremor. Mechanisms of cellular loss and toxicity to the brain and intracranial blood vessels were reviewed. Alcohol works in diverse ways. Short and long term effects on inhibitory GABA and excitatory NMDA Glutamate systems have consequences in alcohol withdrawal. Fetal Alcohol Syndrome can occur as alcohol passes readily through the placenta to the developing fetus.
…………………………………………………………………………………………………
Thank you for your consideration in reading this post. Feedback and suggestions are always welcome
Images and data obtained from sources freely available on the World Wide Web. For educational and information purposes only. This post should not be considered medical or professional advice.
REFERENCES
……………………………….
Deleterious Effects of Alcohol Intoxication: Diminished Cognitive Control and Its Behavioral Consequences
Todd S. Casbon Florida State University
Alan R. Lang Florida State University
John J. Curtin University of Wisconsin
Journal of Abnormal Psychology Copyright 2003 by the American Psychological Association, Inc. 2003, Vol. 112, No. 3, 476–487 0021-843X/03/$12.00 DOI: 10.1037/0021-843X.112.3.476
…………………………………………………..
Alcohol Intoxication Effects on Visual Perception: An fMRI Study
Vince D. Calhoun,1–3* David Altschul,3 Vince McGinty,3 Regina Shih,3
Human Brain Mapping 21:15–25(2004)
……………………………………………………..
Effects of Alcohol Intoxication on Anger Experience and Expression Among Partner Assaultive Men
Christopher I. Eckhardt Purdue University
Journal of Consulting and Clinical Psychology Copyright 2007 by the American Psychological Association 2007, Vol. 75, No. 1, 61–71
………………………………………………………….
The Effects of Alcohol Intoxication and Withdrawal on Hypothalamic Neurohormones and Extrahypothalamic Neurotransmitters
by
András Buzás 1,
Péter Bokor 1,
Biomedicines 2023, 11(5), 1288; https://doi.org/10.3390/biomedicines11051288
Received: 9 February 2023 / Revised: 10 March 2023 / Accepted: 11 April 2023 / Published: 27 April 2023
https://www.mdpi.com/2227-9059/11/5/1288
………………………………………………………………………………
Neurotransmitters in alcoholism: A review of neurobiological and genetic studies
Niladri Banerjee
Amity Institute of Biotechnology, Amity University, Noida, Uttar Pradesh, India
…………………………………………………………………………………….
Increased Glutamatergic Neurotransmission and Oxidative Stress After Alcohol Withdrawal
Guochuan E. Tsai, M.D., Ph.D., Paul Ragan, M.D., Robert Chang, B.S., Shaw Chen, B.S., V. Markku I. Linnoila, M.D., Ph.D., and Joseph T. Coyle, M.D.
https://ajp.psychiatryonline.org/doi/full/10.1176/ajp.155.6.726
…………………………………………………………………………………….
SEROTONIN’S ROLE IN ALCOHOL’S EFFECTS ON THE BRAIN
David M. Lovinger, Ph.D.
…………………………………………………………………………………..
Management of Drug and Alcohol Withdrawal
Thomas R. Kosten, M.D., and Patrick G. O’Connor, M.D., M.P.H.
N Engl J Med 2003;348:1786-95.
Copyright © 2003 Massachusetts Medical Society
…………………………………………………………………………………………
Neuropharmacology of alcohol addiction
V Vengeliene, A Bilbao, A Molander, R Spanagel
First published: 29 January 2009 https://doi.org/10.1038/bjp.2008.30Citations: 392
DOI: 10.1038/bjp.2008.131
https://bpspubs.onlinelibrary.wiley.com/doi/full/10.1038/bjp.2008.30
…………………………………………………………………………………………..
Alcohol and NMDA receptor: current research and future direction
Raman Chandrasekar*
Department of Biochemistry and Biotechnology Core Facility, Kansas State University, Manhattan, KS, USA
………………………………………………………………………………………………..
Pharmacology of Alcohol and Alcohol Use Disorder
Naoyuki Hironaka Reference work entry First Online: 05 November 2022
NeuroPsychopharmacotherapy pp 2505–2524
https://link.springer.com/referenceworkentry/10.1007/978-3-030-62059-2_34
……………………………………………………………………………
GluN2B subunit deletion reveals key role in acute and chronic ethanol sensitivity of glutamate synapses in bed nucleus of the stria terminalis
Tiffany A. Wills, Jason R. Klug, Yuval Silberman, +4 , and Danny G. Winderdanny.winder@vanderbilt.eduAuthors Info & Affiliations
January 4, 2012 109 (5) E278-E287
https://doi.org/10.1073/pnas.1113820109
https://www.pnas.org/doi/10.1073/pnas.1113820109
…………………………………………………………………………………………………
Alcohol Withdrawal Syndrome: Benzodiazepines and Beyond
Psychiatry Section
AnKur SAchdevA1, MonA choudhAry2, MinA chAndrA3
DOI: 10.7860/JCDR/2015/13407.6538
………………………………………………………………………………………………
The Role of the Central Amygdala in Alcohol Dependence
Marisa Roberto, Dean Kirson, and Sophia Khom
Departments of Molecular Medicine and Neuroscience, The Scripps Research Institute, La Jolla, California 92037, USA
Correspondence: mroberto@scripps.edu
Cold Spring Harb Perspect Med 2021;11:a039339
……………………………………………………………………”…………………………
Aug 2012
Effect of Brain Structure, Brain Function, and Brain Connectivity on Relapse in Alcohol-Dependent Patients
Anne Beck, PhD; Torsten Wüstenberg, PhD; Alexander Genauck; et al
Arch Gen Psychiatry. 2012;69(8):842-852. doi:10.1001/archgenpsychiatry.2011.2026
https://jamanetwork.com/journals/jamapsychiatry/fullarticle/1307560
…………………..”?…………..”……………………………………………..
Mechanisms of Ethanol-Induced Cerebellar Ataxia: Underpinnings of Neuronal Death in the Cerebellum
Hiroshi Mitoma Mario Manto and Aasef G. Shaikh
Int. J. Environ. Res. PublicHealth2021,18,8678. https:// doi.org/10.3390/ijerph18168678
……………………………………………………………………………………………
Knowledge atlas of the involvement of glutamate and GABA in alcohol use disorder: A bibliometric and scientometric analysis
Zhanzhang Wang, Xiuqing Zhu, Xiaojia Ni, Yuguan Wen* and
Dewei Shang*
Department of Pharmacy, The Affiliated Brain Hospital of Guangzhou Medical University, Guangzhou China
……………………………………………………………………………
What are signs and symptoms of alcohol withdrawal
Conditions & Diseases by Health Jade Team on August 24, 2017 2.08K views……
……………………………………………………………….l
https://www.mdcalc.com/calc/1736/ciwa-ar-alcohol-withdrawal
CIWA-Ar for Alcohol Withdrawal
…………………………………………………………………
Alcohol-related amnesia and dementia: Animal models have revealed the contributions of different etiological factors on neuropathology, neurochemical dysfunction and cognitive impairment
Ryan P. Vetreno, Joseph M. Hall, and Lisa M. Savage*
Behavioral Neuroscience Program, Department of Psychology, State University of New York
Neurobiol Learn Mem. 2011 November ; 96(4): 596–608. doi:10.1016/j.nlm.2011.01.003.
………………………………………………………………………..
What Happened?
Alcohol, Memory Blackouts, and the Brain
Aaron M. White, Ph.D.
Alcohol Research & Health
……………………………………………………………………….
Mechanism of alcohol-induced oxidative stress and neuronal injury
James Haoraha,*, Servio H. Ramireza, Nicholas Floreania, Santhi Gorantlaa, Brenda Morseya, and Yuri Persidskya,b
aCenter for Neurovirology and Neurodegenerative Disorders, Department of Pharmacology and Experimental Neuroscience, University of Nebraska Medical Center,
Free Radic Biol Med. 2008 December 1; 45(11): 1542–1550. doi:10.1016/j.freeradbiomed.2008.08.030.
…………………………………………………………….
ALCOHOL METABOLISM
Arthur I Cederbaum, PhD
Department of Pharmacology and Systems Therapeutics Mount Sinai School of Medicine
Clin Liver Dis. 2012 November ; 16(4): 667–685. doi:10.1016/j.cld.2012.08.002.
……………………………………………………………
Protein kinase C epsilon mediation of CRF- and ethanol-induced GABA release in central amygdala
Michal Bajo, Maureen T. Cruz, George R. Siggins, +1 , and Marisa Roberto
PNAS June 17, 2008
105 (24) 8410-8415
https://doi.org/10.1073/pnas.0802302105
………………………………………………….
The Rewarding and Anxiolytic Properties of Ethanol within the Central Nucleus of the Amygdala: Mediated by Genetic Background and Nociceptin
Christopher P. Knight, Sheketha R. Hauser,
THE JOURNAL OF PHARMACOLOGY AND EXPERIMENTAL THERAPEUTICS
……………………………………………………..
Alcohol: Effects on Neurobehavioral Functions and the Brain
Marlene Oscar-Berman and
Departments of Anatomy and Neurobiology, Psychiatry, and Neurology, Boston University
Neuropsychol Rev. 2007 September ; 17(3): 239–257. doi:10.1007/s11065-007-9038-6.
………………………………………………………
Mental Illness in Adults With Fetal Alcohol Syndrome or Fetal Alcohol Effects
Chris Famy, B.S., Ann P. Streissguth, Ph.D., and Alan S. Unis, M.D.
Published Online:1 Apr 1998https://doi.org/10.1176/ajp.155.4.552
https://ajp.psychiatryonline.org/doi/full/10.1176/ajp.155.4.552
………………………………………………………..
The Genetics of Alcohol
Metabolism
Role of Alcohol Dehydrogenase and Aldehyde
Dehydrogenase Variants
Howard J. Edenberg, Ph.D.
……………………………………………………………

Leave a comment