
Part 1
ADDICTION PATHWAYS 1
Part 1
Addiction generally follows a progressive course from early exploratory use to compulsion even as it defies precise definition. Here I use terminology in the generally understood sense.
While there is no set boundary there are progressive neurobiological changes which have been observed as early use of addictive substances becomes compulsive with negative impact on health and well being.
This review does not address questions of root causes or treatment outcomes. Neuroscience of addiction is a very new field and many questions remain unanswered. It is an exciting one as recent advances have conclusively demonstrated that there is a biological basis for addiction. This fact alone is a milestone and dispels many myths about drug addiction even as some remain persistent.

This was published in a landmark article in the journal Lancet in 2016. The lead authors were Nora Volkow, chair of the NIDA and George Koob, chair of the NIAAA.
The model describes what happens once the stage of active addiction occurs. It incorporates specific neurobiological pathways with behavior and what is experienced by the individual, principal psychological drives, and neuro adaptive changes.
This is what you get from a general google search for dopamine. There is a lot of hype out there so lets take a look at what dopamine does and does not do.

Dopamine is both a hormone and a neurotransmitter. In the central nervous system it acts as a neurotransmitter involved in reward, mood, memory, and other functions. In the rest of the body it acts in the pancreas, kidneys, GI, cardiovascular and immune systems.

Dopamine is synthesized in many tissues including the nervous system. It is derived from the amino acid tyrosine which is ubiquitous. Tyrosine is a non essential amino acid meaning the body can synthesize it . Tyrosine is converted to l–dopa which is then converted to dopamine. From dopamine we can derive the neurotransmitter / hormones norepinephrine and epinephrine. Together these similar amino acid derivatives are known as catecholamines.
This diagram is what happens in the dopaminergic neuron and synapse. Dopamine is packaged into vesicles. When a signal arrives the vesicles release the neurotransmitter into the synapse. Dopamine docks on receptors on the receiving cell like a key fitting into a lock. The transmitter is then released and taken back up by a transporter to be recycled.
Any of these steps can be altered by neuroadaptive mechanisms or by pharmacological means.
These pathways are tightly regulated. Any change up or down can have significant consequences.
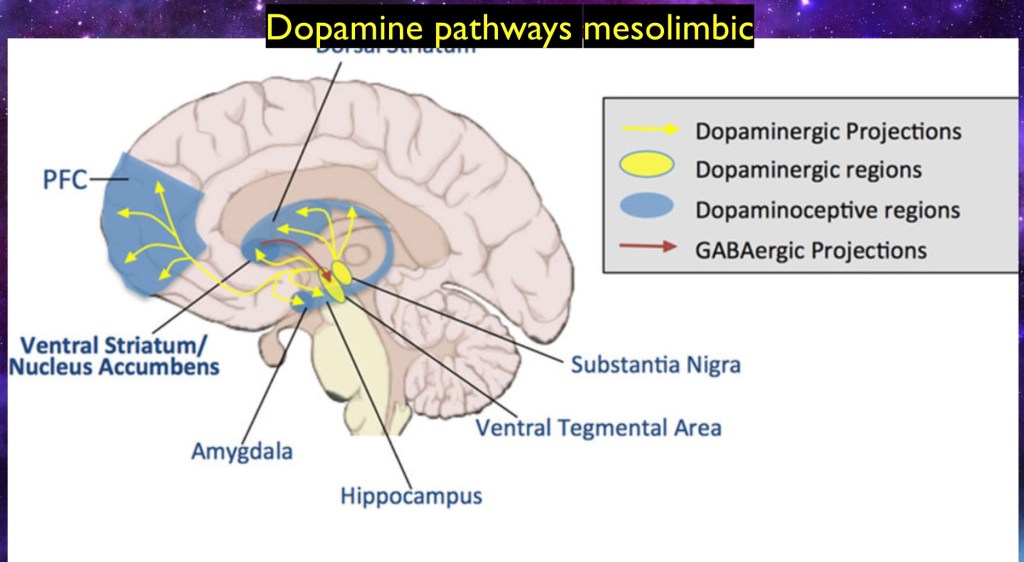
The mesolimbic forward firing dopaminergic pathways are the core of the reward system. The reward response begins in the Ventral Tegmental Area (VTA). This bundle releases dopamine into the Nucleus Accumbens (NAC), the Amyglyla, and the prefrontal Cortex (PFC).
A secondary pathway runs from the Substantia Nigra to the dorsal Striatum. This pathway is important in motor function. It is also active in the reward system.

The reward pathway is how your brain learns that something is good. It is present throughout the animal kingdom. It is essential in learning, motivation and salience.
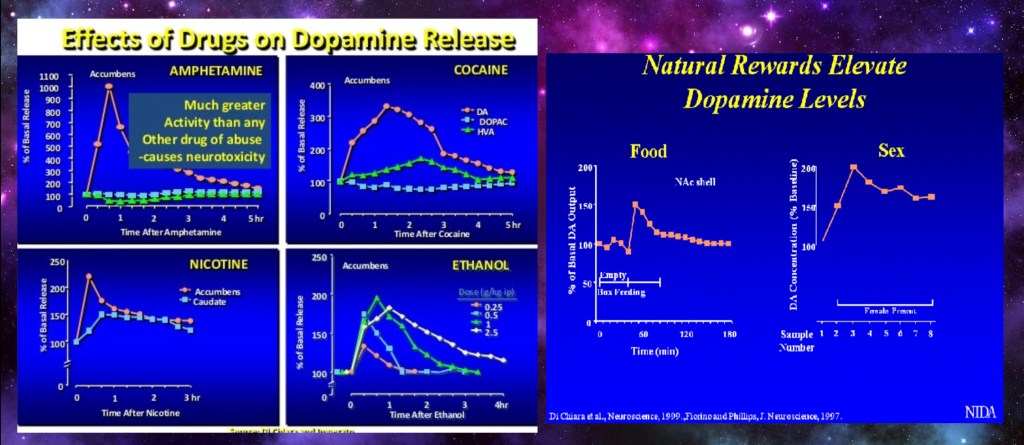
The dopaminergic pathway is activated by any rewarding substance or activity.
These graphs come from animal studies done measuring dopamine levels in the NAC by micro dialysis.
Note that the spike for amphetamine is much higher than the others. Amphetamine peaks at 10x over baseline. The other stimuli are around 2-3 x higher than baseline levels. This is because amphetamines act directly on dopamine neurons. The others act indirectly. This accounts for neurotoxicity seen in amphetamine use.
These levels are measured at the Nucleus Accumbens (NAC) reflecting release originating from the Ventral Tegmental Area (VTA).
This study looked at subjective “high” felt by users given radio labeled cocaine or methylphenidate. Both work by similar mechanisms by blocking dopamine reuptake by the dopamine transporter.
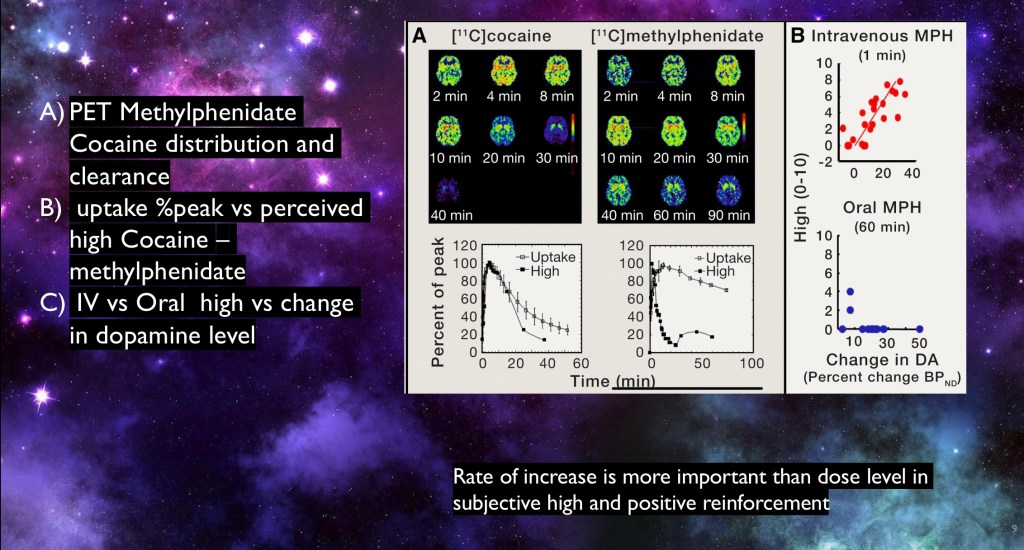
PET of radiolabeled Cocaine and methylphenidate (Ritalin) administered IV. The vertical axis is drug uptake (boxes with bars) and perceived ‘high’ rated by the subjects. Values are expressed as percent of maximum to allow comparison. Note that the hedonic response corresponds to the rate of uptake more that the actual drug level.
- Perceived high, IV vs slower acting oral Methylphenidate. IV Ritalin is often used in experimental studies. The oral form is considered to have some, but low addictive potential.
Subjective reward is a powerful behavioral reinforcer. Faster acting drugs are more rewarding. Fentanyl is one such drug. It has a fast onset and short duration of action.
Dopaminergic pathways also extend to the frontal cortex. This is the thinking part of the brain. Executive function is carried out here. Actions are considered and initiated from the frontal lobe. Short term memory and language also are carried out in this region of the brain.

This study divided subjects into two groups. The control group was naïve to drug use. The second group consisted of chronic cocaine users. They looked at metabolic response by PET using radiolabeled Glucose (FDG).
A) Metabolic activity following IV Methylphenidate. Only areas showing a difference between the two populations are shown. Metabolism is increased in addicted subjects and decreased in controls in the medial orbital frontal cortex. The region shown is involved with emotional processing, salience, and motivation.
- Controls and users demonstrating metabolic changes for placebo and methylphenidate. In addiction there is decreased response to placebo due to learned aversion to associative stimuli not immediately accompanied by drug reward. Cocaine results in increased response compared with controls.
- Perceived desire for drug on vertical axis vs metabolic increases on horizontal axis. Higher frontal cortical metabolism is positively correlated with increased subjective desire for the drug.
These findings indicate a direct relationship between this specific location in the frontal lobe and the ‘high’ perceived by experienced users.
Below is an additional study demonstrating frontal cortical abnormalities occurring in Substance Use Disorder.
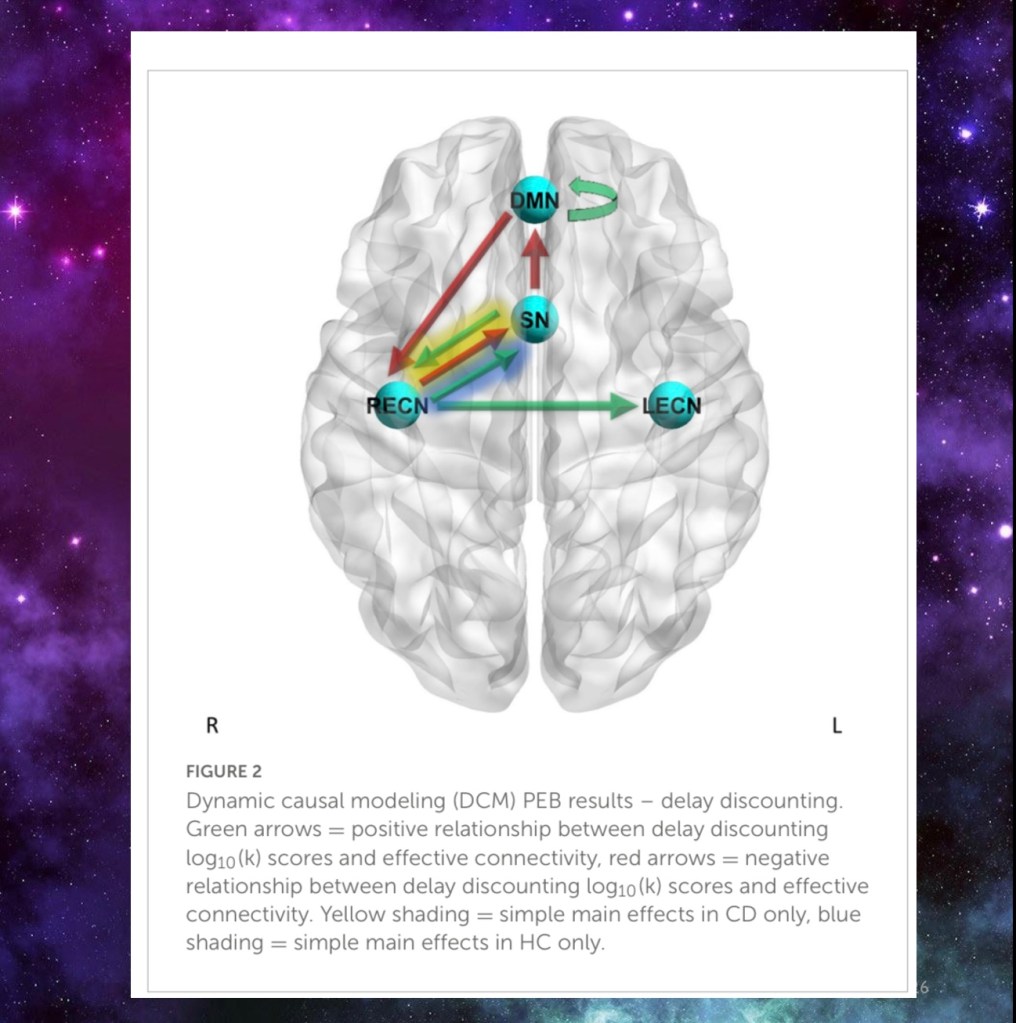
Changes in executive function and impulsivity are well known in addiction. This study used fMRI to map connectivity between different frontal regions in cocaine users and a control cohort.
DMN – default mode network
ECN – executive control network
SN – salience network
HC – healthy controls
CD – cocaine dependent
In the diagram above red arrows indicate negative connectivity. Green arrows indicate positive connectivity.
Delay discounting refers to the tendency to choose smaller immediate rewards over larger delayed rewards.
“Incentive saliency is a cognitive process that grants a “desire” or “want” attribute, which includes a motivational component to a rewarding stimulus.” (Wiki).
Saliency is a key concept in addiction science. It differs from mere “liking”. I like ice cream sundaes too. This differs from active addiction where the substance involves far greater motivation and preoccupation.
The study found decreased connectivity in cocaine users in delay discounting tasks between default and right executive functions, between executive function and saliency, and between saliency and default mode network. These findings demonstrate impaired frontal lobe connectivity between regions critical to salience, motivation, and decision making.
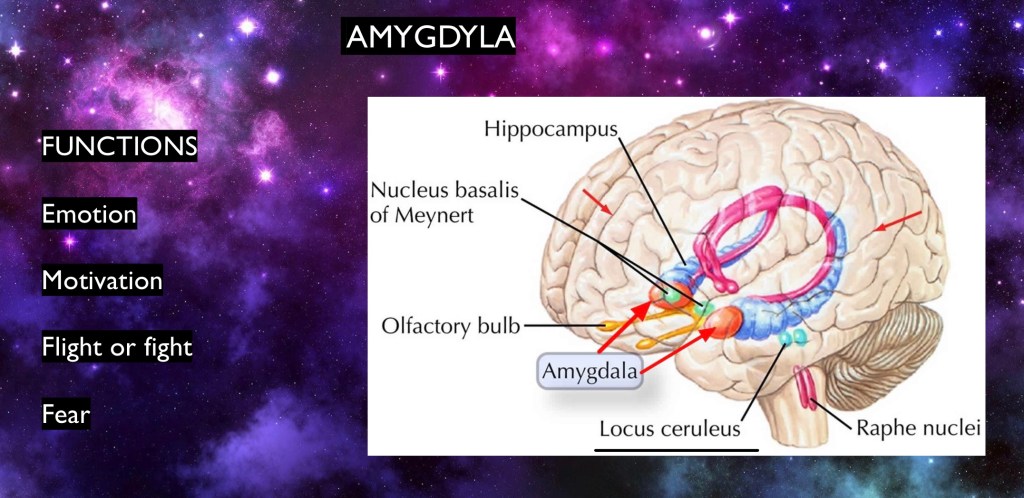
The amygdala is located deep in the base of the brain and can send out signals prior to conscious deliberation by the neocortex. The VTA sends a dopaminergic pathway to the amygdala. From the amygdala there are connections to the frontal lobe and the NA. The amygdala is a critical processing center for emotions and motivation.
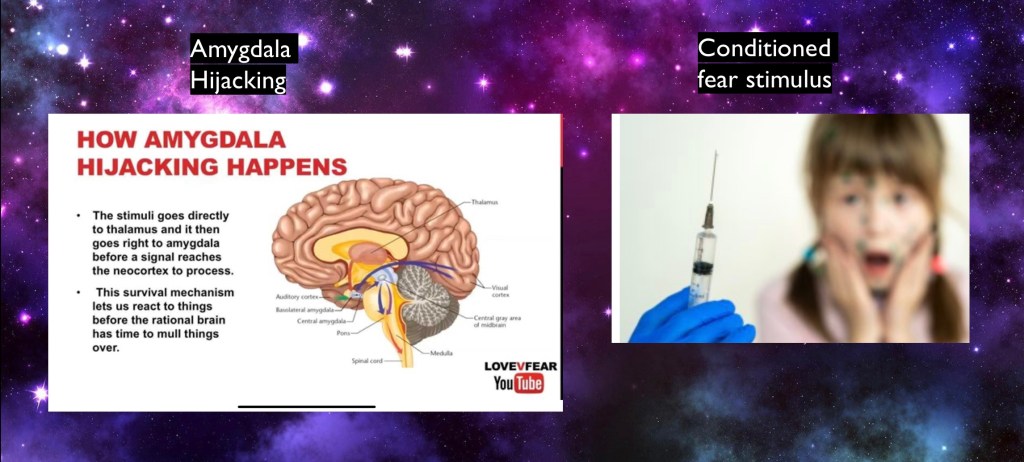
Stress response from the amygdala is increased in addiction and will be further discussed later.
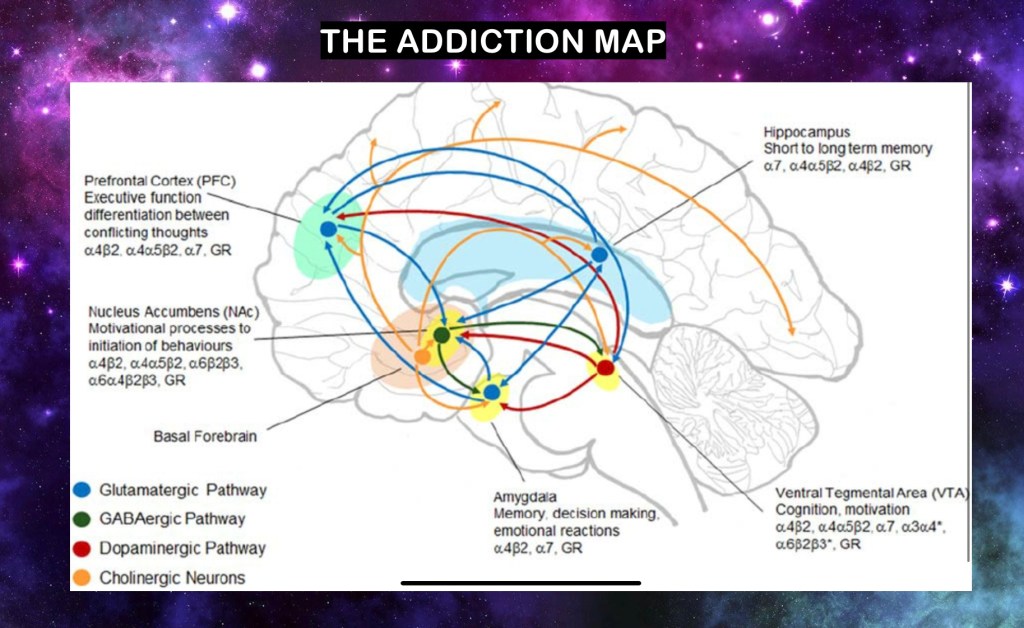
This model looks intimidating. If you break it into parts it shows brain centers we have already been looking at.
The dopamine reward pathway is in red. It is forward firing. It starts at the Ventral Tegmental Area and then to the Nucleus Accumbens. The NA is like the communications hub for the other structures involved.
It also has direct pathways to the Frontal Cortex and the amygdyla
From those centers there are other connections and feedback loops. These can be excitatory Glutamine transmitters shown in blue or inhibitory GABA in green. Additional cholinergic pathways are shown in orange.

Thank you for your time and consideration in reviewing this post. As always any feedback is welcome. References to be included following the next installment.
For educational purposes only. No commercial or institutional interest. This post should not be considered medical or professional advice. Images and data from sources freely available on the World Wide Web..
Jeff K. 5/23

Leave a comment